In the complex world of medical billing, understanding the concept of bill types is essential. Bill type refers to a specific code that classifies the type of services provided, allowing healthcare providers to accurately communicate and process claims with insurance companies. Identifying the correct bill type is crucial for ensuring timely payments and preventing claim denials. In this article, you will gain a clear understanding of what bill types are in medical billing and why they are vital for efficient and accurate reimbursement.
Overview of Medical Billing
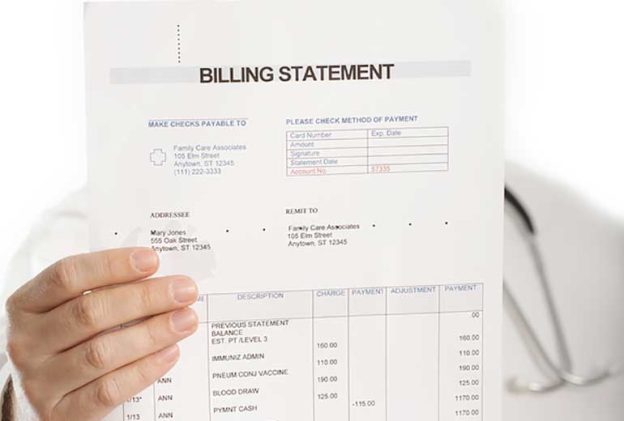
Medical cost concept with stethoscope and medical bill
Definition of medical billing
Medical billing refers to the process of submitting and following up on claims with health insurance companies in order to receive payment for services provided by healthcare providers. It involves translating medical procedures and diagnoses into standardized codes, compiling the necessary documentation, and submitting claims to insurance companies for reimbursement.
Importance of medical billing
Medical billing is a crucial aspect of the healthcare industry as it ensures that healthcare providers receive timely and accurate payment for the services they deliver. Efficient and accurate medical billing practices help to maintain the financial stability of healthcare organizations, allowing them to continue providing quality care to patients. Additionally, medical billing plays a vital role in maintaining compliance with healthcare regulations and ensuring healthcare providers are reimbursed appropriately for the services they render.
Key components of medical billing
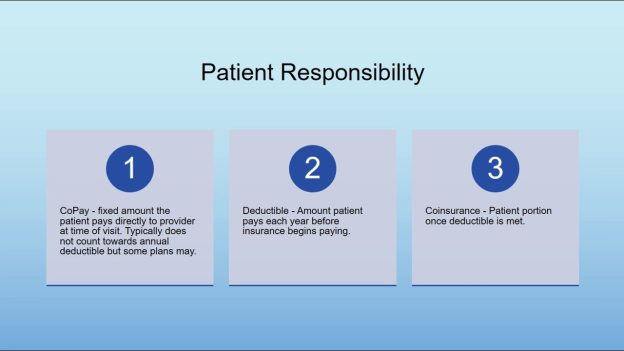
Patient demographics: Medical billing starts with capturing and verifying patient demographic information such as name, address, contact details, and insurance information. Accurate patient information is essential for successful claims submission and reimbursement.
Coding: Medical coding involves assigning specific codes to medical procedures, diagnoses, and services. This ensures that healthcare services are accurately represented, facilitating proper billing and reimbursement processes.
Claim submission: Once coding is completed, medical billing professionals compile all the necessary documentation and submit claims to insurance companies for reimbursement. This includes submitting claims electronically or in paper form, adhering to specific timelines and regulations.
Follow-up and appeals: Medical billing professionals follow up with insurance companies on submitted claims to ensure prompt payment. In cases where claims are denied or not fully reimbursed, professionals may need to file appeals or resubmit claims with additional documentation to secure payment.
Payment posting: Once reimbursement is received from insurance companies, accurate payment posting is crucial. Medical billing professionals match payments to claims, reconcile any discrepancies, and update patient accounts accordingly.
Reporting and analysis: Medical billing also involves generating reports and analyzing billing data to identify trends, measure performance, and identify areas for improvement. This information helps healthcare organizations optimize their billing processes and financial outcomes.
Understanding Bill Types in Medical Billing
Definition of bill type
In medical billing, a bill type refers to a specific code that categorizes the type of healthcare service provided. It categorizes claims based on the setting or type of care, aiding in the reimbursement process and determining the appropriate payment rates.
Why bill types are used in medical billing
Bill types are used in medical billing for several reasons. Firstly, they help insurance companies classify claims and determine the appropriate reimbursement rates for specific services. Secondly, bill types allow healthcare organizations to keep track of the different types of services they provide and analyze reimbursement patterns.
How bill types impact the reimbursement process
Bill types play a significant role in the reimbursement process for healthcare providers. Insurance companies use bill types to determine the reimbursement rates for services rendered by healthcare providers. Each bill type corresponds to a specific payment methodology that outlines the reimbursement rates and guidelines for that particular service category. By assigning the correct bill type, healthcare providers can ensure they are reimbursed correctly and in a timely manner.
Types of Bill Types in Medical Billing
There are various types of bill types in medical billing, each corresponding to a specific type of healthcare service or setting. Understanding these bill types is crucial for accurately coding and billing claims. The following are some of the common bill types in medical billing:
Inpatient bill types
Inpatient bill types are used for services provided to patients who require admission to a hospital or other healthcare facility for a specific period. These bill types are used for comprehensive services, including room charges, ancillary services, surgical procedures, and medications provided during the inpatient stay.
Outpatient bill types
Outpatient bill types are used for services provided to patients who do not require admission to a healthcare facility and receive care on an outpatient basis. These bill types cover services such as clinic visits, diagnostic tests, minor surgical procedures, and outpatient therapies.
Professional bill types
Professional bill types are used for services provided by healthcare professionals that are not performed in a hospital or facility setting. These bill types include services rendered by physicians, nurses, therapists, and other licensed healthcare providers.
Durable Medical Equipment (DME) bill types
Durable Medical Equipment (DME) bill types are used for equipment or supplies that are medically necessary and prescribed by a healthcare provider. These bill types include items such as wheelchairs, oxygen tanks, prosthetic devices, and other durable medical equipment.
Laboratory bill types
Laboratory bill types are used for services provided by clinical laboratories, including blood tests, urine tests, genetic tests, and other laboratory procedures.
Home Health Agency bill types
Home Health Agency bill types are used for services provided to patients in their own homes by home health agencies. These bill types cover services such as skilled nursing care, physical therapy, home health aide services, and medical social services.
Skilled Nursing Facility bill types
Skilled Nursing Facility bill types are used for services provided to patients in skilled nursing facilities. These bill types cover services such as skilled nursing care, rehabilitation therapies, and room charges.
Hospice bill types
Hospice bill types are used for services provided to patients who are in the terminal stages of an illness and receiving hospice care. These bill types cover comprehensive services provided by hospice agencies, including medical care, pain management, counseling, and emotional support.
Ambulatory Surgical Center bill types
Ambulatory Surgical Center bill types are used for services provided in ambulatory surgical centers. These bill types include surgical procedures, diagnostic tests, and other services provided in an outpatient surgical setting.
Other bill types
In addition to the aforementioned bill types, there are various other bill types that cater to specific healthcare services or settings. These include mental health services, radiology services, emergency department services, and more.
Inpatient Bill Types
Definition of inpatient bill types
Inpatient bill types are specific codes used in medical billing to categorize services provided to patients who require admission to a hospital or other healthcare facility for a specific period. Inpatient bill types encompass various charges during the time a patient is admitted, including room charges, ancillary services, surgical procedures, and medications.
Examples of inpatient bill types
Some common examples of inpatient bill types include:
Bill Type 111: Hospital Inpatient Part A General Classification.
Bill Type 121: Hospital Inpatient Part B Inpatient Only for Medical Certification.
Bill Type 131: Hospital Inpatient Part B Inpatient Only.
Reimbursement considerations for inpatient bill types
When submitting claims with inpatient bill types, healthcare providers should ensure that all necessary documentation, including medical records and surgical reports, are included to support the claim. The reimbursement for inpatient services is typically based on a diagnosis-related group (DRG) system, where specific payment rates are assigned based on the patient’s diagnosis, procedures performed, and length of stay. Healthcare providers should accurately code and document these factors to ensure appropriate reimbursement. Additionally, understanding the various rules and regulations associated with inpatient billing, such as Medicare guidelines, is essential to maximize reimbursement for inpatient services.
Outpatient Bill Types
Definition of outpatient bill types
Outpatient bill types are specific codes used in medical billing to categorize services provided to patients who receive care on an outpatient basis, without the need for admission to a healthcare facility. Outpatient bill types include services such as clinic visits, diagnostic tests, minor surgical procedures, therapeutic services, and more.
Examples of outpatient bill types
Examples of outpatient bill types include:
Bill Type 131: Clinic or hospital department visit performed on an outpatient basis.
Bill Type 141: Comprehensive outpatient rehabilitation facility.
Bill Type 151: Hospital outpatient part B only.
Reimbursement considerations for outpatient bill types
Reimbursement for outpatient services is typically based on the Medicare Outpatient Prospective Payment System (OPPS), which assigns payment rates based on specific Current Procedural Terminology (CPT) codes and Ambulatory Payment Classifications (APCs). To ensure correct reimbursement, healthcare providers must accurately code procedures, diagnoses, and other relevant information. Additionally, understanding the specific guidelines and requirements set forth by insurance companies is crucial to avoid claim denials and maximize reimbursement for outpatient services.
Professional Bill Types
This image is property of www.verywellhealth.com.
Definition of professional bill types
Professional bill types are specific codes used in medical billing to categorize services provided by healthcare professionals outside of a hospital or facility setting. These bill types encompass services rendered by physicians, nurses, therapists, and other licensed healthcare providers.
Examples of professional bill types
Examples of professional bill types include:
Bill Type 121: Physician services provided in an inpatient setting.
Bill Type 131: Physician services provided in an outpatient setting.
Bill Type 141: Physical therapy services.
Bill Type 151: Ambulance services.
Reimbursement considerations for professional bill types
The reimbursement for professional services is typically based on the Medicare Physician Fee Schedule (MPFS), which assigns payments based on relative value units (RVUs) and specific conversion factors. Healthcare providers must accurately code procedures, evaluation and management services, and other professional services to ensure appropriate reimbursement. It is important to stay up-to-date with the latest coding guidelines and documentation requirements to maximize reimbursement for professional services.
Durable Medical Equipment (DME) Bill Types
Definition of DME bill types
Durable Medical Equipment (DME) bill types are specific codes used in medical billing to categorize medically necessary equipment or supplies prescribed by a healthcare provider. DME bill types encompass items such as wheelchairs, oxygen tanks, prosthetic devices, and other durable medical equipment.
Examples of DME bill types
Examples of DME bill types include:
Bill Type 121: Prosthetic devices.
Bill Type 131: Medical equipment.
Bill Type 141: Orthotic devices.
Reimbursement considerations for DME bill types
When billing for DME, healthcare providers must ensure that all necessary documentation, including prescriptions and medical necessity forms, are included to support the claim. Reimbursement for DME is typically based on fee schedules or specific payment methodologies set by insurance companies or Medicare. Accurate coding and documentation are crucial to ensuring appropriate reimbursement for DME services.
Laboratory Bill Types
Definition of laboratory bill types
Laboratory bill types are specific codes used in medical billing to categorize services provided by clinical laboratories. These bill types encompass a wide range of laboratory tests and procedures, including blood tests, urine tests, genetic tests, and other laboratory-based diagnostics.
Examples of laboratory bill types
Examples of laboratory bill types include:
Bill Type 110: Independent laboratory testing.
Bill Type 120: Independent laboratory specimen draw.
Bill Type 130: Independent laboratory CLIA waiver.
Reimbursement considerations for laboratory bill types
Reimbursement for laboratory services is typically based on fee schedules or specific payment methodologies set by insurance companies or Medicare. Accurate coding and documentation of laboratory tests, appropriate use of modifiers when necessary, and adherence to specific guidelines are essential for proper reimbursement. Compliance with Clinical Laboratory Improvement Amendments (CLIA) regulations and ensuring proper documentation of medical necessity are also crucial for obtaining reimbursement for laboratory services.
Home Health Agency Bill Types
These bill types encompass a broad spectrum of care, spanning skilled nursing services, physical therapy, home health aide assistance, medical social services, and much more. Accurate and systematic utilization of these bill types is crucial for both healthcare providers and insurance companies to ensure proper reimbursement and transparent record-keeping of the care provided to patients in home health settings.
Definition of Home Health Agency bill types
Home Health Agency bill types are specific codes used in medical billing to categorize services provided to patients in their own homes by home health agencies. These bill types encompass a wide range of services, including skilled nursing care, physical therapy, home health aide services, medical social services, and more.
Examples of Home Health Agency bill types
Examples of Home Health Agency bill types include:
Bill Type 323: Home health – part A.
Bill Type 324: Home health – part B.
Bill Type 329: Parenteral, enteral, and/or nutrition home care.
Reimbursement considerations for Home Health Agency bill types
Reimbursement for home health services is typically based on various factors, including the patient’s health condition, the services provided, and the payment methodology set by insurance companies or Medicare. Accurate coding and documentation of services, adherence to specific guidelines, and regular communication with the involved insurance companies are crucial for maximizing reimbursement for home health services.
Other Bill Types
Each bill type corresponds to a specific category of healthcare services, allowing for efficient and precise billing processes.
Definition of other bill types
Besides the specific bill types discussed above, there are various other bill types that cater to specific healthcare services or settings. These bill types may include mental health services, radiology services, emergency department services, and more.
Examples of other bill types
Examples of other bill types include:
Bill Type 421: Mental health services.
Bill Type 721: Radiology services.
Bill Type 851: Emergency department services.
Reimbursement considerations for other bill types
Reimbursement considerations for these other bill types vary depending on the specific services provided and the payment methodologies set by insurance companies or Medicare. Healthcare providers must accurately code and document these services, ensuring compliance with specific guidelines, and understanding the reimbursement rules associated with each specific bill type to maximize reimbursement. Regular communication and collaboration with insurance companies and payers can help healthcare providers navigate the complexities of reimbursement for these services.
In conclusion, understanding the different bill types in medical billing is critical for accurate coding, billing, and reimbursement processes. From inpatient and outpatient bill types to professional services and specialized bill types for various settings, each category comes with its own unique considerations. Healthcare providers must stay informed about the specific requirements, guidelines, and payment methodologies associated with each bill type to optimize reimbursement and maintain financial stability in the ever-evolving landscape of medical billing.
In the realm of healthcare, a wide range of medical claims exists, serving as crucial tools for patients, healthcare providers, and insurance companies alike. These claims are essential in ensuring that medical services are accurately documented and reimbursed. From primary care visits to surgical procedures, each type of medical claim has its own distinct purpose and intricate process. Understanding the various types of medical claims is not only important for healthcare professionals but also for patients striving for a comprehensive understanding of their medical expenses and insurance coverage. In this article, we will explore the different types of medical claims and shed light on their significance in the complex landscape of healthcare.
Health Insurance Claims
Health insurance claims are an integral part of the healthcare system, allowing individuals to receive reimbursement for the medical services, medication, hospitalization, surgical procedures, and diagnostic tests they have received. Understanding the different types of health insurance claims can help you navigate the process more effectively and ensure that you receive the coverage you are entitled to.
Medical Services Claims
Medical services claims encompass a wide range of healthcare procedures and treatments. These claims include expenses related to physician visits, consultations, laboratory tests, radiology services, and other outpatient services. When submitting a medical services claim, it is important to provide detailed information about the healthcare provider, date of service, and a breakdown of the charges incurred.
Prescription Drug Claims
Prescription drug claims involve the reimbursement of expenses incurred for purchasing medications prescribed by healthcare professionals. Health insurance plans often have different tiers or formularies for prescription drugs, which determine the coverage and cost-sharing arrangement. When submitting a prescription drug claim, it is crucial to provide the name of the medication, dosage, quantity, and the prescribing healthcare provider’s information.
Hospitalization Claims
hospitalization claims cover the expenses associated with inpatient care, including room charges, surgical procedures, nursing care, medications administered in the hospital, and other related services. It is important to thoroughly review your health insurance policy regarding eligibility requirements, coverage limits, and any pre-authorization or pre-certification necessary for hospitalization claims.
Surgical Procedure Claims
Surgical procedure claims pertain to the costs incurred for surgical interventions, such as the surgeon’s fees, anesthesia, operating room charges, and post-operative care. It is essential to gather all relevant documentation, including surgical reports, itemized bills, and any pre-authorization or pre-certification forms, to support your claim for reimbursement.
Diagnostic Test Claims
diagnostic test claims involve reimbursement for the expenses associated with various diagnostic procedures, such as X-rays, MRIs, CT scans, blood tests, and biopsies. Supporting documentation, such as requisition forms, test results, and itemized bills, should be provided when submitting diagnostic test claims.
Workers’ Compensation Claims
Workers’ compensation claims are specific to individuals who have experienced work-related injuries or illnesses. These claims are designed to provide financial assistance and support to employees who have suffered occupational injuries, illnesses, or accidents. Understanding the different types of workers’ compensation claims can help ensure that you receive appropriate compensation for your work-related condition.
Occupational Injury Claims
Occupational injury claims cover injuries sustained while performing work-related tasks or activities. These can include fractures, sprains, strains, burns, cuts, and other physical injuries. It is important to report the injury promptly to your employer, seek appropriate medical treatment, and provide all necessary documentation to support your claim.
Occupational Illness Claims
Occupational illness claims involve illnesses or diseases that are directly related to or caused by exposure to hazardous conditions, substances, or activities in the workplace. These illnesses can range from respiratory conditions, such as asthma and lung disease, to chronic conditions resulting from prolonged exposure to toxic substances. It is crucial to obtain medical documentation linking the illness to your specific work environment when submitting an occupational illness claim.
Workplace Accident Claims
Workplace accident claims are specific to accidents that occur in the work environment, such as slip and falls, machinery accidents, or incidents involving falling objects. These claims may cover expenses related to medical treatment, rehabilitation, lost wages, and disability benefits. Providing detailed documentation of the accident, including witness statements and any applicable incident reports, is essential when filing a workplace accident claim.
Auto Accident Claims
Auto accident claims involve seeking compensation for injuries or damages resulting from motor vehicle accidents. Whether you are a driver, passenger, or pedestrian involved in an auto accident, understanding the different types of auto accident claims can help you navigate the claims process effectively.
Personal Injury Claims
Personal injury claims encompass injuries sustained by individuals involved in motor vehicle accidents. These claims may cover medical expenses, pain and suffering, lost wages, and other damages resulting from the accident. It is essential to gather evidence, such as the accident report, medical records, and witness statements, to support your personal injury claim.
Property Damage Claims
Property damage claims involve seeking reimbursement for damages to your vehicle or other property caused by the accident. These claims cover the costs of repairs or replacement, as well as any related expenses, such as towing or storage fees. Providing photographs of the damage, repair estimates, and any supporting documentation can help facilitate the property damage claims process.
Medical Expenses Claims
Medical expenses claims involve seeking reimbursement for the costs of medical treatment and services resulting from auto accident injuries. These claims cover expenses such as hospital visits, medication, rehabilitation, physical therapy, and other necessary healthcare services. Collecting all relevant medical records, bills, and receipts is crucial when filing a medical expenses claim.
Lost Wages Claims
Lost wages claims pertain to seeking compensation for the income lost due to injuries sustained in an auto accident. These claims cover the wages missed during the recovery period and, in some cases, may extend to future lost earning capacity. It is important to provide documentation, such as pay stubs, tax returns, and a letter from your employer, to support your lost wages claim.
Disability Insurance Claims
Disability insurance claims involve seeking financial assistance and support when an individual is unable to work due to a disability. Understanding the different types of disability insurance claims can help you navigate the claims process and ensure that you receive the benefits you are entitled to.
Short-Term Disability Claims
Short-term disability claims involve seeking benefits for a temporary disability that prevents you from working. These claims typically cover a specific period, such as several weeks to a few months, and provide a percentage of your regular income. Typically, short-term disability claims require medical documentation supporting the disability and its impact on your ability to work.
Long-Term Disability Claims
Long-term disability claims pertain to seeking benefits for a disability that is expected to last for an extended period, usually over six months or more. These claims provide financial support when an individual is unable to perform their job due to the disability. Long-term disability claims often require extensive medical documentation, including physicians’ reports, test results, and evidence of ongoing treatment.
Total Disability Claims
Total disability claims involve seeking benefits when an individual is completely unable to perform any occupation or work due to a disability. These claims typically require rigorous medical documentation and evidence demonstrating the inability to engage in any gainful employment. It is important to thoroughly review your disability insurance policy to understand the criteria for total disability claims.
Partial Disability Claims
Partial disability claims encompass situations where an individual can still perform some work or occupation, but the disability limits their earning capacity. These claims often involve assessing the individual’s residual functional capacity and the impact of the disability on their ability to work. Providing medical documentation and vocational assessments can help support a partial disability claim.
Medical Malpractice Claims
Medical malpractice claims arise when a healthcare professional’s negligence or omission results in harm or injury to a patient. Understanding the different types of medical malpractice claims can help you pursue appropriate legal action and seek compensation for the damages suffered.
Wrong Diagnosis Claims
Wrong diagnosis claims involve situations where a healthcare professional provides an incorrect or delayed diagnosis, leading to harm or injury to the patient. These claims generally require expert testimony to establish the standard of care and prove that the wrong diagnosis caused harm. Medical records, diagnostic tests, and opinions from other healthcare professionals may be crucial when pursuing a wrong diagnosis claim.
Surgical Errors Claims
Surgical errors claims pertain to situations where errors occur during surgical procedures, resulting in harm or injury to the patient. These errors can include wrong-site surgeries, anesthesia errors, instrument or foreign object retention, or other surgical complications. Collecting surgical reports, medical records, and expert opinions is essential when pursuing a surgical errors claim.
Medication Errors Claims
Medication errors claims involve situations where errors occur in prescribing, dispensing, or administering medications, leading to harm or injury to the patient. These claims may cover medication interactions, dosage errors, allergic reactions, or the administration of the wrong medication. It is important to gather all relevant medical records, pharmacy records, and expert opinions when pursuing a medication errors claim.
Birth Injury Claims
Birth injury claims arise when healthcare professionals’ negligence or errors during childbirth lead to harm or injury to the mother or baby. These claims can involve complications during labor, improper use of medical devices, failure to monitor the baby’s well-being, or other birth-related injuries. Collecting detailed medical records, expert opinions, and opinions from specialists can be crucial when pursuing a birth injury claim.
Medicare Claims
Medicare claims pertain to seeking reimbursement for healthcare services covered under the Medicare insurance program. Understanding the different types of Medicare claims can help beneficiaries navigate the complex process and ensure that their expenses are appropriately covered.
Part A Claims
Part A claims involve seeking reimbursement for inpatient hospital services, skilled nursing facility care, hospice care, and some home health services. Medicare Part A claims require submitting the appropriate forms, including itemized bills, physician orders, and other necessary documentation.
Part B Claims
Part B claims encompass reimbursement for outpatient, medical, and durable medical equipment services, including physician visits, laboratory tests, X-rays, and preventive screenings. Beneficiaries need to provide detailed information, including the healthcare provider’s information, service dates, and a breakdown of charges when submitting Part B claims.
Part D Claims
Part D claims involve seeking reimbursement for prescription medications covered under Medicare Part D plans. These claims typically require providing detailed information about the medication, including the name, dosage, quantity, and prescribing physician’s information. It is important to review your Part D plan’s formulary and understand any coverage limitations or cost-sharing arrangements.
Medicaid Claims
Medicaid claims involve seeking reimbursement for healthcare services covered under the Medicaid program, which provides assistance to low-income individuals and families. Understanding the different types of Medicaid claims can help beneficiaries access necessary healthcare services and ensure appropriate coverage.
Inpatient Service Claims
Inpatient service claims cover the expenses associated with hospitalization and other inpatient healthcare services. These claims require submitting detailed documentation, including hospital records, itemized bills, and any necessary authorizations from the Medicaid program.
Outpatient Service Claims
Outpatient service claims involve seeking reimbursement for healthcare services provided outside of a hospital setting, such as physician visits, laboratory tests, and outpatient surgery. Beneficiaries need to provide documentation, such as detailed bills, diagnostic reports, and any referrals or authorizations required by the Medicaid program.
Managed Care Claims
Managed care claims pertain to individuals enrolled in Medicaid managed care plans, where healthcare services are provided through a contracted network of healthcare providers. These claims typically require filing appropriate forms and providing necessary documentation, such as bills, receipts, and any documentation required by the managed care organization.
Veterans Affairs (VA) Claims
Veterans Affairs (VA) claims involve seeking benefits and compensation for injuries or disabilities incurred while serving in the military. Understanding the different types of VA claims can help veterans access the support they are entitled to and navigate the VA claims process.
Service-Connected Claims
Service-connected claims involve seeking benefits for disabilities or injuries directly resulting from military service. These claims require providing evidence linking the disability to the individual’s military service, such as service records, medical evidence, and expert opinions.
Non-Service-Connected Claims
Non-service-connected claims involve seeking benefits for disabilities or injuries that are not directly related to military service. These claims typically involve disabilities acquired after military service or other qualifying circumstances, such as service-connected disabilities impacting an individual’s ability to work.
Disability Pension Claims
Disability pension claims involve seeking financial assistance for veterans who are disabled and have limited income and resources. These claims require demonstrating the veteran’s disability, income limitations, and other eligibility criteria to qualify for a disability pension through the VA.
Eligibility Claims
Eligibility claims encompass situations where veterans seek benefits based on their eligibility for VA programs and services. These claims involve providing necessary documentation, such as discharge papers (DD Form 214), proof of service-connected disabilities, income verification, and other eligibility requirements specific to the VA program or service.
This image is property of i0.wp.com.
Personal Injury Protection (PIP) Claims
Personal Injury Protection (PIP) claims are specific to individuals involved in auto accidents in states with no-fault insurance systems. PIP coverage provides benefits for medical expenses, lost wages, and other related expenses, regardless of who is at fault in the accident. Understanding the different types of PIP claims can help individuals access the available benefits.
Medical Treatment Claims
Medical treatment claims involve seeking reimbursement for medical expenses resulting from an auto accident covered under PIP insurance. These claims typically require providing medical records, bills, and other documentation to verify the necessity and cost of the medical treatment received.
Rehabilitation Claims
Rehabilitation claims pertain to seeking reimbursement for expenses related to physical therapy, occupational therapy, or other rehabilitation services required due to injuries sustained in an auto accident. These claims may require providing treatment plans, invoices, and other documentation to support the need for rehabilitation services.
Lost Income Claims
Lost income claims involve seeking compensation for wages or income lost due to the inability to work following an auto accident covered under PIP insurance. These claims typically require providing evidence of lost wages, such as payroll records, tax returns, and a letter from your employer, to support the claim for lost income.
Funeral Expenses Claims
Funeral expenses claims are specific to situations where a person dies as a result of injuries sustained in an auto accident covered by PIP insurance. These claims provide reimbursement for funeral and burial costs, as well as related expenses such as transportation and handling. Providing itemized funeral bills and other documentation is crucial when filing a funeral expenses claim.
Dental Insurance Claims
Dental insurance claims involve seeking reimbursement for dental services and treatments covered under dental insurance policies. Understanding the different types of dental insurance claims can help individuals access necessary dental care and ensure appropriate coverage.
Preventive Care Claims
Preventive care claims encompass routine dental exams, cleanings, x-rays, and other preventive treatments. These claims typically require providing detailed documentation, such as dental records, service dates, and a breakdown of charges, to support the reimbursement for preventive dental services.
Basic Restorative Claims
Basic restorative claims involve seeking reimbursement for dental procedures aimed at restoring the function and structure of teeth, such as fillings and simple extractions. When filing a basic restorative claim, it is important to provide the dental provider’s information, procedure codes, and a breakdown of charges.
Major Restorative Claims
Major restorative claims pertain to more extensive dental procedures, such as crowns, bridges, dentures, and dental implants. These claims typically require providing treatment plans, diagnostic records, and a breakdown of charges to support the reimbursement for major restorative dental services.
Orthodontics Claims
Orthodontics claims involve seeking reimbursement for orthodontic treatments and braces to correct misaligned or maloccluded teeth. These claims may require pre-authorization or pre-certification and need to be supported by treatment plans, progress reports, and a breakdown of charges to ensure appropriate coverage for orthodontic services.
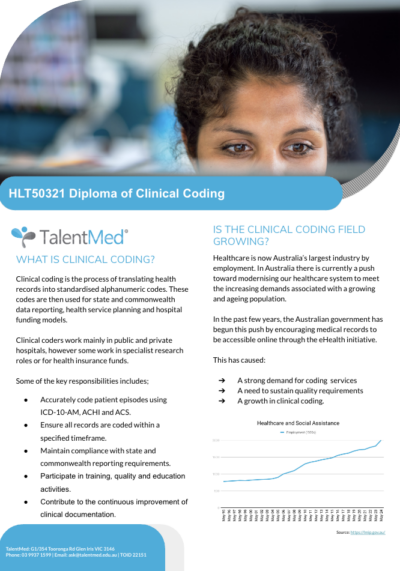
Are you interested in learning clinical coding and are unsure where to start? This article provides a brief overview of how to embark on your journey to mastering this valuable skillset. With the increasing demand for qualified professionals in healthcare information management, learning clinical coding can open up a world of opportunities. By understanding the foundations of clinical coding, gaining practical experience, and investing in continuous learning, you can acquire the expertise necessary to excel in this field. Whether you are a healthcare professional looking to expand your skillset or an aspiring beginner, this article will guide you through the essential steps to become proficient in clinical coding.
Understanding Clinical Coding
What is Clinical Coding?
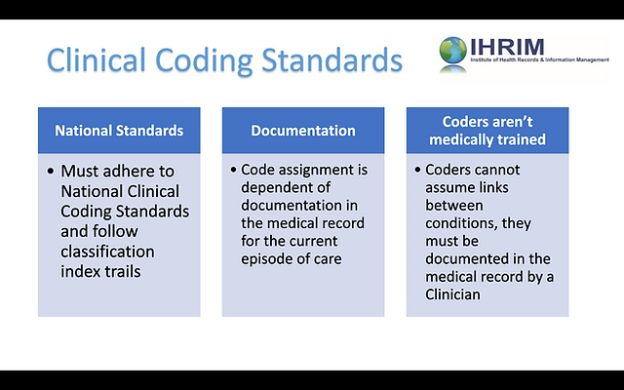
Clinical coding is a process where medical information is transformed into alphanumeric codes for the purpose of documentation, statistical analysis, and reimbursement. These codes represent diagnoses, procedures, treatments, and healthcare services provided to patients. Clinical coders play a crucial role in accurately translating medical information into standardized codes, ensuring the integrity and consistency of healthcare data.
Importance of Clinical Coding
Clinical coding is essential in healthcare for several reasons. Firstly, it enables the collection, analysis, and comparison of data on a local, national, and international level. This data assists in the understanding of disease patterns, healthcare utilization, treatment outcomes, and the effectiveness of interventions. Accurate coding also supports the accurate billing and reimbursement of healthcare services, ensuring that healthcare providers are appropriately compensated for their work. Furthermore, clinical coding plays a vital role in research, public health surveillance, quality improvement initiatives, and policy development.
Role of a Clinical Coder
The role of a clinical coder is significant in the healthcare ecosystem. Clinical coders are responsible for reviewing and analyzing medical records to extract pertinent information and assign appropriate codes following established coding guidelines and principles. They need to have a deep understanding of medical terminology, anatomy, procedures, and clinical documentation. Clinical coders liaise with medical professionals, including doctors and nurses, to clarify any ambiguities or obtain additional information when necessary. They work closely with healthcare administrators, insurance companies, and government agencies to ensure accurate and consistent coding practices across the healthcare system.
Educational Requirements
Background and Skills Required
To pursue a career in clinical coding, a strong background in science, particularly in biology and anatomy, is advantageous. Basic computer literacy and knowledge of medical information systems are also essential. Excellent analytical and critical thinking skills, attention to detail, and the ability to work in a fast-paced environment are crucial for success in this field. Effective communication skills are necessary to interact with healthcare professionals and properly document medical procedures and diagnoses.
Formal Education and Training
While formal education requirements for clinical coding may vary, a post-secondary education in health information management or a related field is commonly preferred by employers. These programs provide comprehensive training in medical coding, anatomy and physiology, medical terminology, health data management, and coding classification systems. Some institutions also offer specialized courses or certificate programs solely focused on clinical coding. It is important to choose an accredited educational program recognized by professional coding associations to ensure quality and validity of the education received.
Certification and Credentialing
Certification Options
Obtaining certification in clinical coding is highly beneficial as it validates the knowledge and competency of a coder. The two main certifications available for clinical coders are the Certified Coding Associate (CCA) and the Certified Coding Specialist (CCS) credentials, both offered by the American Health Information Management Association (AHIMA). The CCA credential is an entry-level certification aimed at individuals who are new to the field or have limited coding experience. The CCS credential, on the other hand, is for experienced coders who specialize in inpatient or outpatient coding.
Benefits of Certification
Obtaining a certification demonstrates a commitment to professional growth and validates one’s expertise in clinical coding. certified coders tend to have higher employability and earning potential compared to non-certified individuals. Additionally, certification provides access to networking opportunities, career advancement prospects, and continuing education resources. Certified coders are often preferred by employers as they have been verified by an industry-recognized governing body, ensuring their competence and adherence to professional standards.
Credentialing Organizations
Apart from AHIMA, several other organizations offer certifications and credentialing opportunities in clinical coding. The American Academy of Professional Coders (AAPC) offers the Certified Professional Coder (CPC) credential, which focuses on outpatient coding. The Board of Medical Specialty Coding (BMSC) offers specialty-specific certifications such as the Certified Cardiology Coder (CCC) and the Certified Orthopedic Surgery Coder (COCS). Credentialing organizations provide a variety of certifications that cater to different coding specialties and levels of experience.
Developing a Study Plan
Setting Goals and Objectives
Before embarking on the journey to become a clinical coder, it is essential to establish clear goals and objectives. Take the time to identify the coding specialization of interest, whether it be inpatient, outpatient, or a specific medical specialty. Determine the desired level of certification and the timeframe within which you would like to achieve it. Setting specific, measurable, achievable, relevant, and time-bound (SMART) goals will help maintain focus and provide direction throughout the learning process.
Choosing Learning Resources
Multiple learning resources are available to aid in the acquisition of clinical coding knowledge. Textbooks, online courses, tutorials, and professional associations are instrumental in providing comprehensive educational materials. It is advisable to choose resources that align with personal learning preferences and accommodate individual schedules and financial constraints. Utilizing a combination of resources, such as textbooks for foundational knowledge and online courses for practical application, can enhance learning outcomes.
Creating a Study Schedule
Organizing and managing time effectively is crucial when pursuing clinical coding education. Creating a study schedule helps allocate dedicated time for learning activities and ensures consistent progress towards the desired goals. Consider the availability of personal time, work commitments, and other responsibilities when designing a study schedule. Prioritize regular study sessions, allow for breaks, and establish realistic expectations to prevent burnout and maintain a healthy work-life balance.
.
Learning Resources and Materials
Textbooks and Reference Guides
Textbooks and reference guides are invaluable resources for clinical coding education. These materials provide in-depth knowledge about medical terminology, anatomy and physiology, coding guidelines, and coding classification systems. Popular titles in the field include “ICD-10-CM and ICD-10-PCS Coding Handbook” by Nelly Leon-Chisen, “CPT Professional Edition” by the American Medical Association, and “Principles of Healthcare Reimbursement” by Anne Casto.
Online Courses and Tutorials
Online courses and tutorials offer flexibility and convenience for individuals seeking clinical coding education. These options provide interactive learning experiences, allowing students to apply coding principles in simulated scenarios. AHIMA and AAPC offer a variety of online courses and self-study materials specifically tailored to coding education. Additionally, numerous e-learning platforms, such as Udemy and Coursera, feature comprehensive clinical coding courses taught by industry professionals.
Professional Associations
Joining professional associations in the field of clinical coding can prove valuable for networking, keeping up with industry updates, and accessing educational resources. AHIMA, AAPC, and the Association of Clinical Coders and Auditors (ACCA) are some renowned professional organizations that provide educational webinars, conferences, and forums for coders to connect and learn from each other. The resources and support provided by professional associations enhance professional development and foster continuous learning among clinical coders.
Hands-On Experience
Internships and Externships
Gaining practical experience through internships and externships can significantly enhance clinical coding skills. Many healthcare facilities, coding consulting firms, and health information management departments offer internships or externships for aspiring coders. These opportunities provide a real-world coding experience, enabling individuals to apply their knowledge in a professional setting under the guidance of experienced coders. Internships and externships also serve as a valuable networking opportunity and may lead to job offers upon completion.
Volunteer Opportunities
Volunteering in healthcare settings, such as clinics or hospitals, can provide exposure to medical records and coding practices. Although volunteers may not have direct coding responsibilities, being immersed in a healthcare environment exposes individuals to medical terminologies, patient encounters, and various healthcare procedures. Observing and engaging with healthcare professionals can deepen understanding of clinical documentation and coding processes, supplementing formal education efforts.
Participate in Case Studies or Research Projects
Engaging in case studies or research projects related to clinical coding offers practical experience and promotes critical thinking skills. Participating in coding audits, where coded records are reviewed for accuracy and compliance, provides valuable feedback and insight into areas of improvement. Case studies involving complex coding scenarios challenge individuals to apply their knowledge and problem-solving abilities. Such experiences sharpen coding skills and facilitate a deeper understanding of coding principles in practical contexts.
Mastering Coding Systems
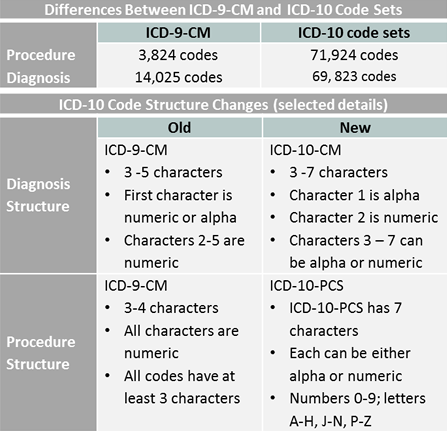
ICD-10-CM
ICD-10-CM (International Classification of Diseases, 10th Revision, Clinical Modification) is a coding system used to classify diseases, injuries, and other health conditions. Mastering ICD-10-CM involves understanding the structure of the code set, the guidelines, and the conventions for accurate code assignment. Extensive knowledge of medical terminology, anatomy, and clinical documentation is crucial to properly assign codes that reflect the patient’s condition.
CPT
Current Procedural Terminology (CPT) is a widely used coding system developed by the American Medical Association. CPT codes are used to describe medical procedures, surgeries, and services provided by healthcare professionals. Mastering CPT involves understanding the organization and structure of the code set, as well as the guidelines and conventions for accurate coding. Familiarity with medical procedures, documentation requirements, and the hierarchy of codes within each section is necessary to accurately assign CPT codes.
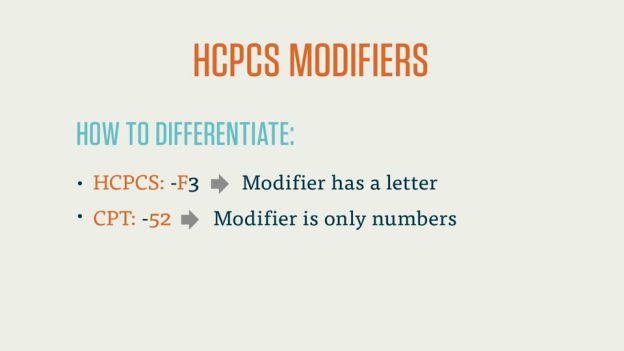
HCPCS
Healthcare Common Procedure Coding System (HCPCS) is a coding system used to describe medical supplies, equipment, and services not covered by CPT codes. HCPCS codes are often used for billing and reimbursement purposes. Mastering HCPCS involves understanding the various code levels, including Level I codes (similar to CPT codes) and Level II codes (specifically for government programs such as Medicare). Awareness of the HCPCS code structure, guidelines, and modifiers is essential for accurate coding and billing.
SNOMED CT
Systematized Nomenclature of Medicine Clinical Terms (SNOMED CT) is a comprehensive clinical terminology and coding system. Unlike other coding systems primarily used in billing and reimbursement, SNOMED CT focuses on clinical documentation and the precise representation of clinical concepts. Mastering SNOMED CT involves understanding the hierarchical structure of the coding system, as well as the principles of concept selection and code assignment. SNOMED CT offers detailed terminology for clinical documentation improvement, research, and quality measurement.
Medical Terminology
Understanding Medical Language
An understanding of medical language is crucial for clinical coders to accurately interpret and code medical information. Medical terminology includes terms for anatomical structures, diseases, symptoms, medications, and procedures. Clinical coders must familiarize themselves with prefixes, suffixes, and root words to comprehend medical terms and derive meaning. Studying medical terminology and its relationship to coding systems enhances coding proficiency and ensures accurate code assignment.
Common Medical Abbreviations
Medical abbreviations are used to efficiently communicate medical information, but they can also pose challenges for clinical coders. Understanding common medical abbreviations is crucial to interpret medical records accurately and assign appropriate codes. A comprehensive list of medical abbreviations is available in textbooks, online resources, and reference guides. Regular exposure to medical abbreviations through coding practice exercises and practical application can improve proficiency in decoding and understanding abbreviations.
Anatomy and Physiology
A strong understanding of human anatomy and physiology is fundamental for clinical coders. Anatomy provides knowledge of the human body’s structure, including organs, systems, and their interrelationships. Physiology helps coders understand the functions of different body systems and how they relate to medical conditions and procedures. Mastery of anatomy and physiology enables clinical coders to accurately assign codes by identifying the specific body areas affected and the underlying pathophysiology of diseases and procedures.
Practical Application
This image is property of www.hccscoding.com.
Coding Practice Exercises
Engaging in coding practice exercises is crucial to reinforce coding skills and improve accuracy and efficiency. Coding exercises can be found in textbooks, online platforms, and coding workbooks specifically designed to provide practical scenarios. These exercises simulate real-life coding scenarios and challenge coders to apply coding guidelines, select appropriate codes, and identify coding errors. Regular practice in coding exercises enhances proficiency and confidence in clinical coding.
Analyzing Medical Records
Analyzing medical records provides hands-on experience in interpreting clinical documentation and assigning codes accordingly. It involves reviewing patient information, such as medical history, diagnostic tests, physician’s notes, and treatment plans. Analyzing medical records strengthens understanding of coding guidelines, reinforces knowledge of medical terms and procedures, and sharpens skills in determining the most accurate and specific codes. This practical application of coding enriches learning outcomes and prepares coders for real-world coding scenarios.
Coding Audits
Coding audits encompass the examination of coded medical records to ensure accuracy and compliance with coding guidelines and regulations. Participating in coding audits provides valuable feedback on coding accuracy, identifies areas for improvement, and deepens understanding of coding principles. Coding audits may be performed internally by healthcare facilities or externally by coding consultants or insurance companies. Engaging in coding audits enhances coding proficiency, promotes quality improvement, and prepares coders for the scrutiny of professional coding organizations.
Continuing Education and Professional Development
Staying Updated with Industry Changes
Clinical coding is a constantly evolving field, with regular updates to coding guidelines, classification systems, and industry standards. Staying updated with industry changes is paramount to ensure accurate and compliant coding practices. Various resources, such as online forums, professional associations, webinars, and newsletters, provide updates on changes, best practices, and emerging trends in clinical coding. Actively seeking opportunities to stay informed and adjusting coding practices accordingly demonstrates commitment to professional growth and excellence.
Attending Seminars and Workshops
Attending seminars and workshops focused on clinical coding allows coders to augment their knowledge and skills. These events provide opportunities to learn from coding experts, delve into specific coding topics, and engage in interactive discussions. Seminars and workshops often include case studies, coding exercises, and practical scenarios to strengthen coding proficiency. Networking with other coders and professionals in the field is an additional benefit of attending such events, as it facilitates knowledge sharing and expands professional networks.
Joining Professional Networks
Joining professional networks, such as local coding associations or online communities, fosters collaboration, learning, and career development. Networking with other clinical coders provides a platform for sharing experiences, seeking advice, and staying updated with coding practices. Professional networks often offer mentoring programs, forums, and job boards, enabling coders to connect with experienced professionals, discuss coding challenges, and explore career opportunities. Active participation in professional networks enhances professional growth and keeps coders informed about the latest coding trends and advancements.
In conclusion, mastering clinical coding requires dedication, a solid educational foundation, practical experience, and continuous professional development. By understanding the significance of clinical coding, pursuing formal education, obtaining certifications, utilizing learning resources, gaining hands-on experience, and engaging in ongoing learning and networking, you can embark on a rewarding career as a skilled clinical coder.
In the field of healthcare, there exists a variety of billing systems that play a crucial role in managing financial transactions. Understanding these systems is vital for healthcare professionals and administrators alike. This article aims to introduce three distinct types of billing systems commonly used in healthcare settings. By exploring the unique features and functionalities of each system, you will gain valuable insights into how these systems optimize billing practices and enhance overall healthcare revenue management. So, let’s dive into the world of billing systems and explore the diverse ways in which healthcare organizations streamline their financial operations.
Traditional Billing System
Definition of Traditional Billing System
The traditional billing system in healthcare refers to the conventional method of invoicing patients for the services rendered by healthcare providers. In this system, paper-based invoices are generated and sent to patients either by mail or in person.
Features of Traditional Billing System
The key features of the traditional billing system include manual data entry, paper-based invoices, and manual payment processing. Healthcare providers manually input patient information, services provided, and associated costs into the billing system. Invoices are then printed and mailed to patients or presented to them during their visit. Payments are received in person or through mail, and manual reconciliation is required.
Advantages of Traditional Billing System
One advantage of the traditional billing system is that it can be easily understood by both healthcare providers and patients due to its simplicity. Additionally, some patients may prefer receiving paper invoices and paying in person rather than through online methods. This system also allows for easy integration with existing manual workflows and infrastructure.
Disadvantages of Traditional Billing System
Despite its advantages, the traditional billing system has several disadvantages. Firstly, it is time-consuming and labor-intensive since it relies heavily on manual data entry and processing. Secondly, the paper-based approach is prone to errors, such as misplaced or lost invoices. Additionally, the delay in receiving payments can negatively impact cash flow for healthcare providers. Finally, the manual reconciliation process can be cumbersome and prone to human error.
Examples of Traditional Billing Systems in Healthcare
Examples of traditional billing systems in healthcare include hospitals that rely on paper invoices and manual payment processing. These facilities often have dedicated departments or staff members responsible for generating and managing the traditional billing system.
Electronic Health Record (EHR) Billing System
Definition of EHR Billing System
The Electronic Health Record (EHR) billing system is a technologically advanced approach to billing in healthcare that leverages electronic medical records to automate and streamline the billing process. This system integrates patient information, services provided, and associated costs directly from electronic health records.
Features of EHR Billing System
Key features of the EHR billing system include automated data entry, electronic invoices, and online payment processing. Healthcare providers enter patient information, services, and costs into the EHR, eliminating the need for manual data entry. Invoices are generated electronically and can be sent to patients via email or made available through patient portals. Online payment options allow for convenient and timely settlements.
Advantages of EHR Billing System
The EHR billing system offers numerous advantages over traditional billing methods. Firstly, it significantly reduces the workload of healthcare providers by automating data entry and invoice generation. Secondly, electronic invoices can be processed and delivered instantly, ensuring faster turnaround times for payments. Additionally, the integration of EHRs with the billing system improves accuracy and reduces errors. Online payment options also enhance convenience for patients.
Disadvantages of EHR Billing System
Despite its advantages, the EHR billing system has some disadvantages. Firstly, implementation or transitioning to an EHR system can be costly and may require staff training. Secondly, technical issues or system downtime can disrupt the billing process. Privacy and security concerns may also arise when transmitting sensitive patient information electronically. Finally, some patients may struggle with technology and prefer traditional methods of receiving and paying invoices.
Examples of EHR Billing Systems in Healthcare
Many healthcare organizations and practices have adopted EHR billing systems. Examples include electronic medical record software providers that offer integrated billing functionalities, as well as hospitals and clinics that have implemented custom EHR systems with integrated billing modules.
Consolidated Billing System
This image is property of cdn-aeclo.nitrocdn.com.
Definition of Consolidated Billing System
The consolidated billing system in healthcare refers to the integration of billing processes for multiple services or healthcare providers into a single, centralized system. This system combines different billing components, such as physician services, laboratory tests, and medications, into one invoice for patients.
Features of Consolidated Billing System
The key features of the consolidated billing system include centralized invoicing, integration of disparate billing components, and comprehensive billing statements. The system consolidates billing information from various sources, eliminating the need for separate invoices. It integrates billing data from different departments or healthcare providers, ensuring a unified invoice for patients. Comprehensive billing statements provide a clear breakdown of charges and services received.
Advantages of Consolidated Billing System
The consolidated billing system offers several advantages. Firstly, it simplifies the billing process for patients by providing a single invoice containing all the services received. This reduces confusion and ensures transparency regarding the overall costs. Secondly, consolidating billing components leads to more accurate and comprehensive statements, avoiding discrepancies or missing charges. Additionally, healthcare providers benefit from streamlined billing operations and reduced administrative burden.
Disadvantages of Consolidated Billing System
Despite its advantages, the consolidated billing system has some disadvantages. Firstly, the consolidation of billing components may result in complex and detailed invoices, which some patients may find overwhelming. Secondly, integrating billing systems from different departments or healthcare providers can be technically challenging and require significant coordination. Lastly, erroneous data entry or mismatched charges can occur during the consolidation process, leading to billing inaccuracies.
Examples of Consolidated Billing Systems in Healthcare
Examples of consolidated billing systems in healthcare include large hospitals or healthcare networks that offer multiple services under one roof. These organizations consolidate billing for services such as consultations, diagnostic tests, procedures, and medications into a single invoice for patients.
Episode-of-Care Billing System
Definition of Episode-of-Care Billing System
The episode-of-care billing system is a method of billing healthcare services based on a specific medical event or condition. Instead of charging per individual service, this approach groups related services into a single package, covering the entire episode of care from diagnosis to treatment.
Features of Episode-of-Care Billing System
Key features of the episode-of-care billing system include bundled billing, comprehensive care packages, and standardized pricing. Instead of separately billing for each service, healthcare providers combine relevant services, such as consultations, tests, procedures, and follow-up visits, into one package. These comprehensive care packages ensure that all necessary treatments are included and simplify the billing process. Standardized pricing helps establish consistent costs for each episode of care.
Advantages of Episode-of-Care Billing System
The episode-of-care billing system offers several advantages. Firstly, it promotes cost transparency by providing patients with a comprehensive package price upfront. This reduces confusion and allows patients to budget accordingly. Secondly, bundled billing incentivizes efficiency and encourages coordination among healthcare providers, resulting in improved care quality. Additionally, standardized pricing facilitates comparative analysis and benchmarking of treatment costs.
Disadvantages of Episode-of-Care Billing System
Despite its advantages, the episode-of-care billing system has some disadvantages. Firstly, determining the appropriate services to include and pricing for each episode can be complex and require extensive coordination among healthcare providers. Secondly, unforeseen complications or variations in patient conditions may necessitate additional services or treatments not initially bundled, potentially affecting costs. Lastly, some patients may prefer itemized billing to understand the breakdown of charges for each service.
Examples of Episode-of-Care Billing Systems in Healthcare
Examples of episode-of-care billing systems in healthcare include bundled payment models for specific procedures or conditions, such as joint replacements or maternity care. In these models, healthcare providers offer a bundled package covering all necessary services related to the episode of care, including pre-operative consultations, surgery, post-operative care, and rehabilitation.
Alternative Payment Models (APM) Billing System
This image is property of www.businessintegrityservices.com.
Definition of APM Billing System
The Alternative Payment Models (APM) billing system is a payment approach that deviates from the traditional fee-for-service model. APMs aim to incentivize value-based care and quality outcomes by linking reimbursement to patient outcomes or cost savings.
Features of APM Billing System
Key features of the APM billing system include value-based reimbursement, quality metrics, and risk-sharing arrangements. Instead of paying for individual services, healthcare providers receive payments based on the quality of care delivered and patient outcomes. APMs often include performance metrics tied to quality indicators or cost savings targets. Risk-sharing arrangements allocate financial responsibility among healthcare payers and providers, encouraging collaboration.
Advantages of APM Billing System
The APM billing system offers several advantages. Firstly, it incentivizes healthcare providers to focus on delivering high-quality care and achieving positive patient outcomes rather than simply providing more services. This shift towards value-based care can lead to improved patient satisfaction and better long-term health outcomes. Secondly, APMs encourage collaboration and coordination among healthcare providers by sharing financial risks, fostering a more integrated approach to care delivery.
Disadvantages of APM Billing System
Despite its advantages, the APM billing system has some disadvantages. Firstly, implementing and transitioning to APMs can be challenging and require significant changes to existing billing and care delivery models. Secondly, defining accurate quality metrics and determining fair reimbursement can be complex. Additionally, risk-sharing arrangements may lead to financial uncertainties for healthcare providers, especially in cases where target outcomes or cost savings are not attained.
Examples of APM Billing Systems in Healthcare
Examples of APM billing systems in healthcare include accountable care organizations (ACOs) and bundled payment models. ACOs focus on coordinating care for a defined population, with payments tied to meeting quality and cost targets. Bundled payment models, as mentioned earlier, reimburse healthcare providers based on the entire episode of care, promoting value-based and coordinated care.
Subscription-Based Billing System
Definition of Subscription-Based Billing System
The subscription-based billing system in healthcare involves patients paying a fixed recurring fee to access a range of healthcare services over a specified period. This approach allows patients to receive comprehensive care without the need for individual service-based billing.
Features of Subscription-Based Billing System
Key features of the subscription-based billing system include recurring fees, access to bundled services, and membership benefits. Patients pay a predetermined amount on a regular basis, typically monthly or annually, to access a wide range of healthcare services. These services may include regular check-ups, preventive care, and selected treatments. Membership benefits might include priority access, discounted rates, or additional services beyond the subscription coverage.
Advantages of Subscription-Based Billing System
The subscription-based billing system offers several advantages. Firstly, it promotes preventive care and ongoing health management by providing patients with regular access to healthcare services. This model encourages patients to seek care proactively, leading to early detection and better disease management. Secondly, the fixed recurring fee helps patients budget for their healthcare expenses more precisely. Additionally, membership benefits can enhance patient experience and loyalty.
Disadvantages of Subscription-Based Billing System
Despite its advantages, the subscription-based billing system has some disadvantages. Firstly, patients who require infrequent medical care may find the recurring fee unnecessary or costly. Secondly, there may be limitations or additional charges for certain services not covered by the subscription. Lastly, patients may be required to commit to a subscription term, potentially limiting their freedom to choose alternative healthcare providers or treatments.
Examples of Subscription-Based Billing Systems in Healthcare
Examples of subscription-based billing systems in healthcare include concierge medicine practices and direct primary care models. These models typically offer patients access to a comprehensive range of primary care services for a fixed, recurring fee. Patients can benefit from increased access to personalized care, extended appointment times, and enhanced physician-patient relationships.
Outsourced Billing System
In the dynamic realm of healthcare administration, the use of outsourced billing systems has emerged as a strategic solution. These systems involve the delegation of billing processes to specialized third-party service providers, offering healthcare providers relief from administrative burdens. By exploring the features, advantages, and potential drawbacks of outsourced billing systems, healthcare professionals can make informed decisions regarding this transformative approach to billing.
Let’s delve into the key elements of outsourced billing systems in healthcare, shedding light on how they enhance efficiency, optimize revenue, and simplify the complexities of the billing landscape.
Definition of Outsourced Billing System
The outsourced billing system in healthcare involves utilizing third-party billing services to handle the billing processes on behalf of healthcare providers. This system allows healthcare providers to delegate billing tasks to specialized companies, relieving them of the administrative burden.
Features of Outsourced Billing System
Key features of the outsourced billing system include third-party providers, comprehensive billing services, and improved efficiency. Healthcare providers partner with specialized billing companies that offer end-to-end billing services. These services include patient data management, claims submission, payment processing, and follow-up on outstanding receivables. By outsourcing these tasks, healthcare providers can focus on patient care while benefiting from increased billing efficiency.
Advantages of Outsourced Billing System
The outsourced billing system offers several advantages. Firstly, it allows healthcare providers to offload the administrative burden of billing and focus on their core competency of providing patient care. Secondly, specialized billing companies often have extensive experience and expertise in navigating complex billing regulations, minimizing billing errors and maximizing reimbursement rates. Additionally, outsourcing can lead to improved billing efficiency, reducing claim denials and accelerating payment cycles.
Disadvantages of Outsourced Billing System
Despite its advantages, the outsourced billing system has some disadvantages. Firstly, entrusting billing tasks to an external party may create concerns related to privacy and security of patient data. Healthcare providers need to ensure proper contractual agreements and data protection measures are in place. Secondly, coordination and communication between the healthcare provider and the billing company are crucial to avoid miscommunications or delays in the billing process. Lastly, outsourcing can come with additional costs, which healthcare providers need to consider when deciding on the financial viability of the arrangement.
Examples of Outsourced Billing Systems in Healthcare
Examples of outsourced billing systems in healthcare include medical billing service providers, revenue cycle management companies, and healthcare consulting firms. These companies offer comprehensive billing solutions and expertise to healthcare providers, enabling them to streamline their billing processes and improve financial performance.
Self-Pay Billing System
n the ever-evolving landscape of healthcare finance, the self-pay billing system has emerged as a crucial avenue for patients and providers alike. This system places the responsibility of payment directly on patients, bypassing insurance providers or third-party payers. It offers a unique set of features and benefits that cater to individuals without insurance or those seeking more control over their healthcare expenses.
Definition of Self-Pay Billing System
The self-pay billing system in healthcare involves patients directly paying for their services without involving insurance providers or third-party payers. This system applies to patients who do not have insurance coverage or choose to pay out-of-pocket for healthcare services.
Features of Self-Pay Billing System
Key features of the self-pay billing system include direct patient payments, customization of service costs, and flexible payment options. In this system, patients are responsible for paying the full cost of their healthcare services at the time of service. Service costs can be customized based on individual patients’ needs and financial capabilities. Flexible payment options, such as installment plans or discounts for upfront payments, may be offered to facilitate affordability.
Advantages of Self-Pay Billing System
The self-pay billing system offers several advantages. Firstly, it eliminates the complexity associated with insurance claims and third-party reimbursement, streamlining the billing process for healthcare providers. Secondly, patients without insurance coverage can receive healthcare services without the need to navigate insurance requirements or worry about claim denials. Additionally, offering flexible payment options improves accessibility to care for individuals who may not have insurance or face financial limitations.
Disadvantages of Self-Pay Billing System
Despite its advantages, the self-pay billing system has some disadvantages. Firstly, patients may find it challenging to afford the full cost of healthcare services without the support of insurance coverage. This could deter individuals from seeking necessary care or lead to financial hardships. Secondly, healthcare providers may face challenges in determining service costs and pricing structures, as they need to strike a balance between affordability and maintaining sustainable financial operations.
Examples of Self-Pay Billing Systems in Healthcare
Examples of self-pay billing systems in healthcare include cash-only clinics, cosmetic or elective procedure centers, and certain specialty practices. These providers cater to patients who are not covered by insurance or who prefer to pay out-of-pocket for specific services, such as aesthetic treatments or alternative therapies.
Third-Party Billing System
This image is property of www.outsourceaccelerator.com.
Definition of Third-Party Billing System
The third-party billing system in healthcare involves billing services being facilitated by an intermediary, such as insurance companies or government payers. This system is commonly used to process healthcare claims and manage reimbursements.
Features of Third-Party Billing System
Key features of the third-party billing system include submission of claims, adjudication of claims, and reimbursement processes. Healthcare providers submit claims to the third-party payer, providing details of the services rendered and associated costs. The payer then reviews the claims, verifying eligibility, adherence to coverage guidelines, and accurate coding. Upon approval, the payer reimburses the healthcare provider based on predetermined rates or negotiated agreements.
Advantages of Third-Party Billing System
The third-party billing system offers several advantages. Firstly, it provides a standardized and efficient approach to claim processing for healthcare providers. By outsourcing the billing process, healthcare providers can focus on patient care while relying on the expertise of the third-party payer. Secondly, patients benefit from the convenience of not having to pay the full cost upfront and can access covered services without the financial burden.
Disadvantages of Third-Party Billing System
Despite its advantages, the third-party billing system has some disadvantages. Firstly, healthcare providers may face challenges related to claim denials, delayed reimbursements, or disputes over coding and reimbursement rates. Secondly, coordinating billing processes with multiple third-party payers can be administratively demanding and require specialized expertise. Additionally, limited control over reimbursement rates may impact the financial viability of certain services or procedures.
Examples of Third-Party Billing Systems in Healthcare
Examples of third-party billing systems in healthcare include insurance companies, managed care organizations, and government payers, such as Medicare or Medicaid. These entities act as intermediaries between healthcare providers and patients, managing the billing and reimbursement processes for covered services.
Conclusion
In conclusion, the healthcare industry offers a range of billing systems to accommodate various operational needs and the evolving landscape of healthcare delivery. The traditional billing system, despite its simplicity, can be time-consuming and prone to errors. On the other hand, electronic health record (EHR) billing systems leverage technology to streamline the billing process and improve accuracy. The consolidated billing system integrates various services into a single invoice, simplifying the billing experience for patients. The episode-of-care billing system bundles related services for specific medical events, promoting cost transparency and quality outcomes. Alternative payment models (APM) incentivize value-based care and quality outcomes, shifting the focus from fee-for-service. Subscription-based billing systems offer comprehensive care packages for a recurring fee, while outsourced billing systems relieve healthcare providers of administrative burdens. Self-pay billing systems cater to patients paying directly for services, while third-party billing systems involve intermediaries like insurance companies or government payers. Each system has its advantages and disadvantages, highlighting the complexity and diversity of billing in healthcare. Healthcare providers must carefully evaluate their needs and consider the best fit to ensure optimal financial performance and patient satisfaction.
Clinical coding is a specialized field that plays a vital role in healthcare. In this article, we will explore the path to becoming a clinical coder, including the necessary skills, education, and certifications required for success. By understanding the journey and requirements involved, you will gain valuable insights into this rewarding career and be equipped to embark on your own professional development in clinical coding.
Education and Qualifications for becoming a clinical coder
Becoming a clinical coder requires a solid educational foundation. The following are the steps you can take to obtain the necessary education and qualifications for this profession:
Obtain a high school diploma
The first step towards becoming a clinical coder is to obtain a high school diploma or equivalent. A high school education provides a strong foundation in basic subjects such as mathematics, English, and science, which are essential for understanding complex medical coding concepts.
Complete a postsecondary certificate program
After obtaining a high school diploma, you can enroll in a postsecondary certificate program in medical coding. These programs typically provide specialized coursework in medical terminology, anatomy, physiology, coding guidelines, and electronic health records management. Completing a certificate program will equip you with the necessary knowledge and skills to enter the field of clinical coding.
Earn an associate degree
While a postsecondary certificate is the minimum requirement for entry-level positions in clinical coding, earning an associate degree in health information technology or a related field can significantly enhance your job prospects. An associate degree program typically includes coursework in medical coding, health information management, database management, and healthcare ethics. Additionally, earning an associate degree demonstrates your dedication and commitment to advancing your knowledge and skills in clinical coding.
Pursue a bachelor’s degree
Although not required for entry-level positions, pursuing a bachelor’s degree in health information management or a related field can open doors to advanced roles in clinical coding and provide opportunities for career growth. A bachelor’s degree program delves deeper into topics such as healthcare information systems, quality improvement, reimbursement methodologies, and legal and ethical considerations in healthcare. This level of education prepares you for leadership roles and provides a comprehensive understanding of the healthcare industry as a whole.
Certification requirements
Certification is often preferred and sometimes required by employers in the field of clinical coding. Here are the steps you need to follow to obtain certification as a clinical coder:
Understand the different coding certifications
There are several coding certifications available, each with its own focus and requirements. The most widely recognized coding certifications include the Certified Professional Coder (CPC) credential, offered by the American Academy of Professional Coders (AAPC), and the Certified Coding Specialist (CCS) credential, offered by the American Health Information Management Association (AHIMA). It is important to familiarize yourself with the different certifications available and their specific requirements to determine which one is most suitable for your career goals.
Choose the appropriate certification
Once you have a clear understanding of the different certifications available, you can choose the one that aligns with your career aspirations and meets the requirements set by potential employers in your desired work setting. Consider factors such as the focus of the certification, the organization offering it, and any prerequisites or experience requirements.
Study for the certification exam
Once you have chosen the appropriate certification, it is important to dedicate time and effort to study for the certification exam. This may involve reviewing coding guidelines, practicing coding scenarios and exercises, and familiarizing yourself with the specific content areas covered in the exam. Consider utilizing study resources such as textbooks, online courses, practice exams, and study guides to enhance your preparation.
Pass the certification exam
Passing the certification exam is the final step in obtaining certification as a clinical coder. The exam assesses your knowledge and understanding of coding principles, guidelines, and best practices. It is important to arrive at the exam well-prepared, confident, and familiar with the exam format and requirements. Once you pass the exam, you will receive your certification, which serves as a validation of your coding expertise and can significantly enhance your job prospects in the field.
This image is property of www.stepintothenhs.nhs.uk.
Gaining coding experience
In addition to education and certification, gaining practical coding experience is essential for becoming a successful clinical coder. Here are some avenues for gaining coding experience:
Internship or on-the-job training
Many healthcare organizations offer internships or on-the-job training programs for aspiring clinical coders. These programs provide hands-on experience under the guidance of experienced professionals, allowing you to apply your knowledge and skills in a real-world setting. Participating in an internship or training program can not only enhance your coding skills but also provide valuable networking opportunities and potential job offers.
Volunteer opportunities
Consider volunteering your coding services at healthcare facilities, community clinics, or nonprofit organizations. Volunteering not only allows you to gain practical coding experience but also demonstrates your commitment to giving back to the community and can be a valuable addition to your resume. Look for opportunities where you can work alongside experienced coders who can provide guidance and mentorship.
Part-time or entry-level coding positions
Starting in a part-time or entry-level coding position can provide you with the necessary experience to grow in the field. These positions may offer opportunities to work with more experienced coders, learn from their expertise, and gain exposure to a variety of coding scenarios. While these positions may not be as lucrative as advanced roles, they serve as stepping stones towards future career growth.
Networking and professional associations
Building a strong professional network is crucial for gaining coding experience and staying abreast of industry developments. Joining professional associations such as the AAPC or AHIMA can provide access to networking events, industry conferences, and educational resources. Networking with experienced coders and attending industry events can help you discover job opportunities, gain valuable insights, and establish relationships that can contribute to your professional growth.
Medical terminology forms the foundation of clinical coding. Familiarize yourself with medical terminology related to anatomy, physiology, and diseases to accurately translate medical diagnoses and procedures into appropriate codes. This knowledge will ensure accurate coding and facilitate effective communication with healthcare providers.
Understanding coding guidelines and systems
To effectively code medical records, it is essential to stay updated on the latest coding guidelines and systems, such as the International Classification of Diseases (ICD) and Current Procedural Terminology (CPT). Familiarize yourself with the coding conventions, rules, and conventions specific to each coding system to ensure accurate and consistent coding practices.
Proficiency in coding software and tools
Clinical coding involves the use of specialized coding software and tools, such as encoding software and electronic health record systems. Develop proficiency in using these tools to navigate through medical records, assign appropriate codes, and ensure data accuracy and integrity. Staying updated on advancements in coding technology and software applications is also important to maintain a competitive edge in the field.
Attention to detail and accuracy
Coding requires meticulous attention to detail and a focus on accuracy. Every code assigned must be carefully selected based on the specific documentation in the medical record. Cultivate a mindset of precision, double-check your work, and develop methods to ensure accuracy and completeness. Attention to detail is crucial to maintain the integrity and quality of coded data.
This image is property of talentmed.edu.au.
Keeping up with industry updates
The field of clinical coding is constantly evolving, with new coding guidelines, best practices, and regulations introduced regularly. To stay current in this dynamic field, you need to continuously update your knowledge and skills. Here are some strategies to keep up with industry updates:
Continuing education and professional development
Continuing education is a key component of professional growth as a clinical coder. Stay informed about continuing education options, such as workshops, seminars, and online courses that focus on the latest coding developments. Allocate time and resources to participate in these educational opportunities to expand your knowledge and stay updated on industry trends.
Participate in coding workshops and conferences
Coding workshops and conferences provide valuable opportunities to learn from industry experts, network with fellow coders, and gain exposure to cutting-edge coding techniques and technologies. Participating in these events can broaden your perspective, enhance your coding skills, and keep you informed about the latest industry advancements.
Subscribe to industry publications and websites
Subscribe to reputable industry publications and websites that provide updates on coding guidelines, regulatory changes, and industry trends. These resources serve as valuable references and keep you informed of any changes that may impact your coding practices. Regularly reading these publications will help you stay current and informed in the field.
Join online coding communities
Online coding communities, such as forums and social media groups, provide a platform for coders to connect, share experiences, and seek advice. Engaging with these communities can help you stay updated on coding trends, access coding resources, and learn from the experiences of other coders. Actively participate in discussions, ask questions, and share your knowledge to benefit from the collective wisdom of the coding community.
Practical tips for aspiring clinical coders
Here are some practical tips to help you succeed in your journey towards becoming a clinical coder:
Develop strong analytical and problem-solving skills
Clinical coding requires the ability to analyze complex medical records, identify relevant information, and apply coding concepts accurately. Developing strong analytical and problem-solving skills will enable you to navigate through challenging coding scenarios and make informed decisions. Practice critical thinking and problem-solving exercises to sharpen these skills.
Practice coding exercises and case studies
Repetition and practice are key to mastering coding skills. Regularly engage in coding exercises and case studies to improve your coding accuracy, speed, and efficiency. Work with a variety of medical records to gain exposure to different coding scenarios and develop versatility in your coding skills.
Stay organized and manage time effectively
Being organized and managing your time effectively are crucial in the fast-paced field of clinical coding. Develop systems and strategies to organize your workload, prioritize tasks, and meet deadlines. Efficient time management and organizational skills will help you optimize your productivity and ensure accurate and timely coding.
Seek feedback and guidance from experienced coders
Seeking feedback and guidance from experienced coders can help you identify areas for improvement and gain valuable insights. Establish relationships with more experienced coders and request feedback on your coding work. Actively listen to their advice and learn from their experiences to enhance your coding skills and professional growth.
This image is property of static.wixstatic.com.
Advancing in the field
Becoming a clinical coder opens up various opportunities for advancement and specialization. Here are some ways to advance in the field:
Specialize in a specific area of coding
Consider specializing in a specific area of coding to enhance your expertise and career prospects. Specializations could include inpatient coding, outpatient coding, professional fee coding, or coding for a specific medical specialty. By becoming an expert in a particular area, you can position yourself for higher-level roles and increase your earning potential.
Pursue advanced certifications
Earning advanced coding certifications can significantly enhance your credentials and open doors to advanced career opportunities. Advanced certifications such as the Certified Professional Coder-Hospital Outpatient (CPC-H) credential or the Certified Coding Specialist-Physician-Based (CCS-P) credential demonstrate your proficiency in specific coding areas and increase your marketability.
Gain experience in leadership roles
Expand your skill set and increase your market value by exploring leadership roles within the coding field. Opportunities may exist to become a coding supervisor, coding manager, or coding consultant. Leadership roles not only offer higher earning potential but also provide the chance to shape and influence coding practices within organizations.
Continuing education for career growth
Continuing education should not stop once you have obtained your initial coding certification. Stay committed to lifelong learning by pursuing additional education and professional development opportunities. This could include earning a master’s degree in health information management or pursuing industry certifications and credentials in related fields such as healthcare administration or revenue cycle management. Advanced education and certifications can pave the way for executive-level positions and expanded career opportunities.
Job search and employment opportunities
After obtaining the necessary education, certification, and experience, you can begin your job search in the field of clinical coding. Here are some strategies to increase your chances of finding employment:
Prepare a well-crafted resume and cover letter
Write a targeted resume and cover letter that highlight your education, certifications, and relevant experience. Tailor your resume and cover letter to the specific job requirements and emphasize your coding skills, attention to detail, and ability to accurately translate medical records into codes.
Utilize online job boards and professional networks
Utilize online job boards and professional networking platforms to search for job openings in the clinical coding field. Post your resume on relevant job sites and join coding-related groups and forums to expand your professional network. Networking can often lead to job opportunities or recommendations from fellow coders.
Attend job fairs and career events
Job fairs and career events provide opportunities to connect with potential employers and explore job openings in the coding field. Dress professionally, bring copies of your resume, and be prepared to engage with recruiters and hiring managers. Networking at these events can help you establish valuable connections and gain insights into the job market.
Develop a strong online presence
Create a strong online presence by establishing a professional LinkedIn profile and showcasing your coding skills, certifications, and experience. Engage in online discussions, share relevant articles, and connect with industry influencers. A strong online presence can attract the attention of potential employers and provide opportunities for career advancement.
This image is property of d3njjcbhbojbot.cloudfront.net.
Salary and career outlook
Clinical coding offers promising career prospects with competitive salaries. However, several factors can impact your salary and career progression:
Research the salary ranges for clinical coders
Research the salary ranges in your geographical area to gain an understanding of the average compensation for clinical coders. Factors such as education, experience, certifications, job location, and the type of healthcare organization can influence salary levels. Salary surveys and industry reports can provide valuable insights into prevailing pay rates.
Consider factors that affect salary
Factors such as specialization, advanced certifications, and experience in leadership roles can significantly impact your earning potential as a clinical coder. By gaining expertise in a specific coding area or pursuing advanced certifications, you can position yourself for higher paying positions and increase your value within the job market.
Explore career advancement opportunities
Clinical coding offers diverse career advancement opportunities. By continuously updating your skills, pursuing higher levels of education, and seeking leadership roles, you can progress in your career and increase your salary potential. Keep an eye out for opportunities to take on more responsibility, manage coding teams, or contribute to strategic initiatives within healthcare organizations.
Stay updated on industry trends and demand
Staying abreast of industry trends and demand is important for long-term career planning. Monitor developments in healthcare regulations, coding guidelines, and reimbursement methodologies to anticipate changes that may impact job availability and salary levels. Continuously seek opportunities to expand your knowledge and skills in response to industry demands.
Conclusion
Becoming a clinical coder requires a combination of education, certification, practical experience, and continuous professional development. By following the steps outlined in this article, you can set yourself on the path to a rewarding career in clinical coding. Remember to stay committed to lifelong learning, stay current with industry updates, and pursue opportunities for specialization and career advancement. The field of clinical coding offers diverse career opportunities and the potential for personal and professional growth. Embrace the challenge, seek out mentorship, and be persistent in pursuing your goals as you embark on this exciting career path.
In the realm of healthcare, billing systems play a crucial role in the financial operations of medical facilities. Understanding the various types of billing systems is essential for healthcare providers to efficiently manage and accurately process patient payments. This article examines three distinct billing systems commonly utilized in the healthcare industry, shedding light on their functionalities, advantages, and potential drawbacks. By delving into the intricacies of these billing systems, healthcare professionals can enhance their billing processes while ensuring compliance with industry standards and regulations.
This image is property of cdn-aeclo.nitrocdn.com.
Overview of Billing Systems in Healthcare
Billing systems in healthcare play a crucial role in the financial management of healthcare organizations. These systems are designed to accurately process and generate bills for the services rendered to patients. By utilizing different billing systems, healthcare providers can streamline their revenue cycle management and ensure timely reimbursement for their services. In this article, we will explore the different types of billing systems used in healthcare, their key features, advantages, disadvantages, and their role in the future of healthcare billing.
Fee-for-Service Billing System
The fee-for-service billing system is one of the most common billing systems used in healthcare. Under this system, healthcare providers charge patients based on the services provided or procedures performed. Each service or procedure is assigned a specific fee, and the final bill is calculated by multiplying the fee with the quantity of services rendered.
Key Features
The key features of the fee-for-service billing system include:
Service-Based Billing: Charges are calculated based on the specific services rendered to the patient.
Individual Pricing: Each service or procedure has its own predetermined fee.
Flexibility: Healthcare providers have the freedom to choose and perform services as needed.
Advantages
The fee-for-service billing system offers several advantages, including:
Financial Incentives: Providers have the potential to earn more revenue by performing more services.
Patient Flexibility: Patients have the freedom to choose their healthcare providers and services.
Disadvantages
Despite its advantages, the fee-for-service billing system has some disadvantages, including:
Fragmented Care: Providers may focus on maximizing their revenue rather than coordinating care effectively.
Cost Inflation: Unnecessary services may be performed to increase revenue, leading to higher healthcare costs.
Capitation Billing System
The capitation billing system is an alternative approach to healthcare billing where healthcare providers are paid a fixed, per-member-per-month fee for the services they provide to a specific group of patients, regardless of the actual services rendered. This system aims to promote cost-effective care and better coordination among healthcare providers.
Key Features
The key features of the capitation billing system include:
Fixed Payments: Providers receive a predetermined payment for each patient assigned to them.
Population Health Management: Providers are incentivized to provide preventive and coordinated care to improve patient outcomes.
Advantages
The capitation billing system offers several advantages, including:
Cost Control: Providers are motivated to deliver efficient and cost-effective care to maximize their profit margins.
Quality Improvement: Coordinated care and population health management can lead to improved patient outcomes.
Disadvantages
However, there are also some disadvantages to the capitation billing system, including:
Inadequate Reimbursement: Providers may receive fixed payments that do not sufficiently cover the costs of providing care.
Incentive Misalignment: Providers may prioritize cost savings over necessary treatments, potentially compromising patient care.
Bundled Payment Billing System
The bundled payment billing system is a payment model where healthcare providers receive a single payment for a specific episode of care, which includes all the services and procedures related to that episode. This system aims to incentivize providers to deliver coordinated and efficient care.
Key Features
The key features of the bundled payment billing system include:
Episode-Based Payments: Providers receive a single payment for the entire episode of care.
Care Coordination: Providers are encouraged to collaborate to ensure efficient and high-quality care.
Advantages
The bundled payment billing system offers several advantages, including:
Cost Savings: Providers are motivated to streamline care delivery and reduce unnecessary services or procedures.
Quality Improvement: Care coordination and collaboration among providers can lead to improved patient outcomes.
Disadvantages
However, there are also some disadvantages to the bundled payment billing system, including:
Financial Risk: Providers may bear financial losses if the cost of care exceeds the bundled payment amount.
Limited Scope: This system may not be suitable for all types of healthcare services and may require customization for different specialties.
This image is property of www.businessintegrityservices.com.
Resource-Based Relative Value Scale (RBRVS) Billing System
The Resource-Based Relative Value Scale (RBRVS) billing system is a widely used method of determining the payment for medical services based on the resources required to perform those services. It assigns relative values to different services based on factors such as physician work, practice expense, and malpractice insurance.
Key Features
The key features of the RBRVS billing system include:
Relative Value Units (RVUs): Services are assigned specific RVUs based on the resources involved in providing them.
Conversion Factor: RVUs are multiplied by a conversion factor to calculate the payment for a particular service.
Advantages
The RBRVS billing system offers several advantages, including:
Standardization: It provides a standardized method for determining the payment for medical services.
Transparency: The RVU-based payment system allows for more transparency in billing and reimbursement.
Disadvantages
However, there are also some disadvantages to the RBRVS billing system, including:
Complexity: The calculation of RVUs and the conversion factor can be complex and may require specialized knowledge.
Potential Inaccuracy: The system may not always accurately reflect the resources required to provide a specific service.
Prospective Payment System (PPS)
The Prospective Payment System (PPS) is a reimbursement methodology used primarily by government payers like Medicare and Medicaid. Under this system, predetermined payment rates are established for specific healthcare services or procedures based on various factors such as diagnosis, procedure codes, and patient characteristics.
Key Features
The key features of the Prospective Payment System (PPS) include:
Diagnosis-Related Groups (DRGs): Services are categorized into DRGs, each associated with a predetermined payment rate.
Fixed Payments: Providers receive a predetermined payment based on the patient’s diagnosis and the assigned DRG.
Advantages
The Prospective Payment System (PPS) offers several advantages, including:
Cost Predictability: Providers can anticipate and plan their revenues based on the established payment rates.
Incentive for Efficiency: Providers are motivated to deliver cost-effective care to maximize their revenue.
Disadvantages
However, there are also some disadvantages to the Prospective Payment System (PPS), including:
Potential Underpayment: The fixed payment rates may not adequately cover the cost of providing certain healthcare services.
Limited Flexibility: Providers may face challenges if the predetermined payment rates do not align with the actual costs incurred.
Electronic Billing Systems
Electronic billing systems, also known as e-billing systems, utilize electronic documentation and processing to streamline the billing and reimbursement process in healthcare. These systems replace paper-based billing with electronic records, making it more efficient, accurate, and secure.
Benefits
The benefits of electronic billing systems include:
Improved Efficiency: Electronic billing systems automate various billing processes, reducing manual tasks and saving time.
Enhanced Accuracy: These systems minimize human errors and ensure accurate billing and claims processing.
Cost Savings: Electronic billing systems eliminate paper-related expenses and reduce administrative costs.
Implementation Challenges
While electronic billing systems offer numerous benefits, there are also implementation challenges to consider, including:
Infrastructure Requirements: Healthcare organizations need the necessary infrastructure and technology to support electronic billing systems.
Training and Adoption: Healthcare providers and staff must be trained to effectively use and adapt to electronic billing systems.
Management and Evaluation of Billing Systems
Efficiency Assessment
Efficiency assessment is a crucial aspect of managing billing systems in healthcare. It involves analyzing key performance indicators (KPIs) such as claim acceptance rates, denial rates, and revenue collection to identify areas for improvement. Regular monitoring and evaluation help identify bottlenecks and optimize the billing process for maximum efficiency.
Risk Management
Effective risk management is essential in billing systems to mitigate potential compliance and financial risks. This involves implementing controls, policies, and procedures to prevent fraud, abuse, and billing errors. Regular audits and internal reviews can help identify and address potential risks in billing practices.
Compliance Monitoring
Billing systems must comply with various regulations and guidelines, such as the Health Insurance Portability and Accountability Act (HIPAA) and the Centers for Medicare and Medicaid Services (CMS) guidelines. Compliance monitoring ensures adherence to these regulations, minimizing the risk of penalties and legal issues. Regular education and training on compliance requirements are also essential for billing system management.
This image is property of www.outsourceaccelerator.com.
Billing Systems and Revenue Cycle Management
Billing systems play a critical role in revenue cycle management (RCM), which involves the financial aspects of patient care from registration to final payment. Integrating billing systems with other RCM components such as patient registration, charge capture, and claims processing streamlines the entire revenue cycle and ensures timely reimbursement.
Workflow Optimization
Optimizing workflows in billing systems improves efficiency and reduces errors in claim submission and payment processing. Workflow optimization includes automating manual tasks, standardizing processes, and utilizing technology to streamline communication and data exchange between different departments involved in the billing process.
Claims Processing
Effective claims processing is a fundamental function of billing systems in healthcare organizations. This involves verifying patient eligibility, submitting accurate and timely claims to payers, and managing denials and appeals. Efficient claims processing ensures proper reimbursement and minimizes revenue leakage.
Future Trends in Healthcare Billing Systems
Value-based Care and Alternative Payment Models
The future of healthcare billing systems is shifting towards value-based care and alternative payment models. These models focus on quality outcomes and incentivize providers to deliver high-value care. Instead of volume-based fee-for-service payments, providers may be reimbursed based on the quality, efficiency, and effectiveness of care provided.
Artificial Intelligence and Automation
Artificial intelligence (AI) and automation are poised to revolutionize healthcare billing systems. AI-powered algorithms can analyze large volumes of data, identify patterns, predict billing errors, and automate claim submission and payment processes. This not only improves accuracy and efficiency but also frees up resources for more complex tasks.
Interoperability and Data Integration
Interoperability and data integration are key drivers for the future of healthcare billing systems. Seamless exchange of patient data between different healthcare systems and payers improves billing accuracy, reduces administrative burden, and enhances the overall patient experience. Standardized data exchange protocols and interoperable systems will be crucial for achieving this goal.
In conclusion, billing systems in healthcare play a vital role in revenue cycle management and ensure timely reimbursement for healthcare services. The various types of billing systems, such as fee-for-service, capitation, bundled payment, RBRVS, and PPS, offer different approaches to billing and reimbursement. Electronic billing systems provide numerous benefits, but their implementation requires careful planning and consideration of infrastructure and training requirements. Efficient management, evaluation, and integration of billing systems are crucial for effective revenue cycle management. The future of healthcare billing systems lies in value-based care, AI, automation, interoperability, and data integration, which will shape the way healthcare services are billed and reimbursed.
To embark on a career as a clinical coder, there are various steps that you can undertake to ensure both a successful transition and long-term growth in this field. This article will provide a comprehensive overview of the necessary qualifications, skills, and experience required to become a clinical coder. By understanding the path that lies ahead, you will be equipped with the knowledge needed to navigate the intricate world of healthcare coding and contribute to the accuracy and efficiency of medical records.
Education and Training
Obtain a High School Diploma
To become a clinical coder, it is essential to start with a solid educational foundation. The first step is to obtain a high school diploma or its equivalent. A high school education provides the necessary basic knowledge and skills required for further education and training in the field of clinical coding.
Pursue a Bachelor’s Degree
While a high school diploma is the minimum requirement, many employers prefer candidates who have pursued higher education. Pursuing a bachelor’s degree in health information management or a related field can provide a more comprehensive understanding of healthcare practices and coding systems. A bachelor’s degree program typically covers topics such as medical coding, health information management, healthcare ethics, and data analysis.
Consider a Certification Program
In addition to a bachelor’s degree, completing a certification program in clinical coding is highly recommended. Certificate programs in clinical coding provide specialized training and focus on the specific coding systems and practices used in the field. These programs can be completed in a shorter timeframe compared to a bachelor’s degree and can enhance your job prospects and demonstrate your commitment to the field.
Develop Essential Skills
Attention to Detail
As a clinical coder, attention to detail is paramount. You will be responsible for accurately assigning codes to medical procedures, diagnoses, and other healthcare services. One small error in coding can have significant consequences for healthcare providers, insurance companies, and patients. Developing keen attention to detail will ensure that you accurately translate medical information into codes.
Analytical Skills
Analytical skills are crucial in clinical coding as you will need to analyze medical records, identify relevant information, and assign the appropriate codes. Being able to navigate complex medical documentation and identify the key pieces of information requires strong analytical thinking. Additionally, the ability to identify coding patterns and trends can help you become more efficient and accurate in your coding processes.
Medical Terminology
A solid understanding of medical terminology is essential for clinical coders. Knowledge of medical terms, anatomy, and physiology helps in accurately interpreting and translating medical documentation into codes. Familiarizing yourself with common medical terms, their abbreviations, and their context within medical records will significantly enhance your coding abilities.
Gain Clinical Experience
This image is property of d3njjcbhbojbot.cloudfront.net.
Internships
Internships provide valuable practical experience in a healthcare setting and can be a stepping stone towards a career in clinical coding. Seek out opportunities to intern at hospitals, medical clinics, or other healthcare facilities where you can observe and learn from experienced clinical coders. Internships allow you to apply your knowledge in a real-world setting and gain insight into the day-to-day responsibilities of a clinical coder.
Volunteer Work
Volunteering in healthcare-related organizations or clinics can also help you gain valuable exposure to the medical field. While you may not have direct coding responsibilities as a volunteer, being part of a healthcare team allows you to observe the coding process and understand the larger healthcare system. This hands-on experience will help you better understand the intricacies of clinical coding and its importance in healthcare delivery.
Shadowing
Shadowing experienced clinical coders is another excellent way to gain insight into the profession. By observing and learning from professionals already working in the field, you can gain practical knowledge on coding techniques, software usage, and documentation review. Shadowing experiences can be arranged through networking or by reaching out to professionals in the field or your local medical coding association.
Become Familiar with Medical Coding Systems
ICD-10
ICD-10 (International Classification of Diseases, Tenth Revision) is the primary coding system used by clinical coders worldwide. It provides a standardized set of codes for diseases, conditions, injuries, and procedures. Developing familiarity with ICD-10 coding guidelines, conventions, and structure is essential to accurately assign codes.
CPT
CPT (Current Procedural Terminology) codes are used to classify medical, surgical, and diagnostic procedures and services provided by healthcare professionals. Clinical coders must be familiar with the CPT coding system to accurately assign codes to procedures and services performed in medical settings. Understanding CPT coding rules and guidelines will ensure accurate and consistent coding practices.
HCPCS
HCPCS (Healthcare Common Procedure Coding System) is a coding system used primarily for Medicare and Medicaid claims. It includes codes for medical supplies, equipment, and services not covered by CPT codes. Familiarizing yourself with HCPCS codes will expand your coding knowledge and enable you to code a broader range of services.
Understand Health Insurance and Billing Practices
This image is property of www.stepintothenhs.nhs.uk.
Knowledge of Insurance Policies
To be an effective clinical coder, you need to have a solid understanding of health insurance policies and coverage. Familiarize yourself with the different types of insurance plans, coverage limitations, and reimbursement processes. This knowledge will enable you to navigate insurance requirements and accurately code procedures and services for appropriate reimbursement.
Understanding of Reimbursement Systems
Clinical coders play an essential role in ensuring accurate reimbursement for healthcare services. Understanding different reimbursement systems, such as fee-for-service, prospective payment systems, and diagnosis-related groups, is crucial. This knowledge will allow you to assign the appropriate codes that align with the specific reimbursement systems and guidelines.
Stay Updated with Industry Changes
Continuing Education
The field of clinical coding is constantly evolving, with regular updates to coding guidelines, regulations, and systems. It is crucial to stay updated with the latest changes and advancements in the industry. Participating in continuing education programs, workshops, and seminars will help you stay informed and maintain your proficiency in clinical coding.
Professional Development
Engaging in professional development activities is essential for career growth and staying updated with industry trends. Joining webinars, attending conferences, and reading industry publications will expose you to new coding techniques, emerging technologies, and best practices. Actively seeking out opportunities to enhance your professional skills will make you a more competent and competitive clinical coder.
Join Professional Organizations
This image is property of www.northwestcareercollege.edu.
AAPC
Consider joining professional organizations such as the AAPC (American Academy of Professional Coders). Membership in organizations like AAPC offers access to valuable resources, networking opportunities, and specialized training programs. These organizations provide a platform for interaction with other professionals, allowing you to exchange knowledge, stay updated, and foster professional relationships.
AHIMA
Another reputable professional organization in the field of clinical coding is AHIMA (American Health Information Management Association). AHIMA offers numerous resources, educational programs, and certifications that can support your professional growth. Becoming a member of AHIMA can provide access to industry-leading publications, networking events, and opportunities to contribute to the advancement of the field.
Prepare for Certification Exams
Review Study Materials
Certification exams are typically required to become a clinical coder. To prepare for these exams, it is crucial to review relevant study materials. Look for study guides, textbooks, and online resources that cover the exam topics comprehensively. Ensure that you allocate sufficient time for studying and create a study plan to cover all the necessary content.
Take Practice Tests
Taking practice tests is an effective way to assess your knowledge and build confidence before the actual certification exam. Practice tests help you become familiar with the format of the exam, identify areas where you may need additional study, and simulate the exam environment. Utilize available practice test resources to gauge your readiness and make any necessary adjustments to your study approach.
Obtain Certification
Pass the Certification Exam
Obtaining certification is a significant milestone in becoming a clinical coder. Certification exams are typically administered by professional coding organizations such as AAPC and AHIMA. These exams assess your knowledge and competence in clinical coding. By passing the exam, you demonstrate your proficiency and dedication to maintaining high coding standards.
Maintain Certification
Certification in clinical coding typically requires ongoing education to maintain its validity. Stay informed about continuing education requirements and complete the necessary courses or workshops to ensure your certification remains active. Additionally, participating in professional development activities and staying updated with industry changes will enhance your skills and maintain your professional standing.
Seek Employment Opportunities
Apply for Clinical Coding Positions
Once you have gained the necessary education, training, and certification, it’s time to apply for clinical coding positions. Look for job openings in hospitals, physician offices, insurance companies, and other healthcare organizations. Tailor your resume to highlight your relevant education, clinical experience, and certifications. Emphasize your attention to detail, analytical skills, and knowledge of coding systems to stand out to potential employers.
Utilize Networking
Networking can be a powerful tool in securing employment opportunities. Attend industry conferences, join online forums and communities, and actively seek connections with other clinical coders or healthcare professionals. Networking can provide valuable insights, job leads, and recommendations that can help you advance your career in clinical coding.
Consider Remote or Freelance Work
Remote or freelance work opportunities are increasingly available in the field of clinical coding. Consider exploring these options to expand your job prospects and gain valuable experience. Remote coding allows you to work from the comfort of your home, providing flexibility and eliminating geographic constraints. Freelancing can expose you to a variety of coding projects and environments, helping you develop diverse skills.
In conclusion, becoming a clinical coder requires a solid educational foundation, mastery of coding systems, and practical clinical experience. By obtaining the necessary education and certifications, developing essential skills, and staying up-to-date with industry changes, you can embark on a successful career in clinical coding. Remember to seek out employment opportunities, utilize networking, and consider remote or freelance work to further enhance your professional journey as a clinical coder.
If you have ever wondered about pursuing a career in healthcare that combines analytical skills with attention to detail, becoming a clinical coder might be the ideal path for you. Clinical coders play a crucial role in accurately translating medical diagnoses and procedures into a coded format. In this article, explore the steps and requirements to embark on this rewarding profession, as well as the skills and knowledge necessary to excel in the field of clinical coding. Discover the diverse opportunities available and the potential for professional growth in this challenging yet essential healthcare role.
Education and Training
High School Education
To become a clinical coder, a solid foundation in education is essential. It starts with completing high school, where you should focus on subjects such as biology, chemistry, mathematics, and computer science. These subjects lay the groundwork for the knowledge and skills needed for the field of clinical coding. A strong academic performance during high school will give you a competitive edge when pursuing further education and training in this field.
Undergraduate Degree
While not always mandatory, obtaining an undergraduate degree can significantly enhance your chances of becoming a successful clinical coder. Pursuing a degree in health information management, medical coding, or a related field will provide you with a deep understanding of medical terminology, coding systems, and healthcare administration. A comprehensive undergraduate program will also cover courses in anatomy, physiology, data management, and computer information systems, further preparing you for a career as a clinical coder.
Clinical Coding Courses
After completing your undergraduate degree, it is essential to undertake specialized clinical coding courses. These courses focus specifically on medical coding practices, coding guidelines, and the use of industry-standard coding systems, such as the International Classification of Diseases (ICD) and the Current Procedural Terminology (CPT). These courses will equip you with the necessary skills to accurately assign codes to medical diagnoses, procedures, and services based on clinical documentation.
Certification Programs
To demonstrate your expertise and enhance your job prospects, pursuing certification in clinical coding is highly recommended. There are several organizations that offer certification programs, most notably the American Health Information Management Association (AHIMA) and the American Academy of Professional Coders (AAPC). These certification programs typically require passing a rigorous exam to assess your coding knowledge and skills. By becoming certified, you will showcase your commitment to excellence and increase your chances of securing desirable employment opportunities in the healthcare industry.
Required Skills and Qualities
Attention to Detail
As a clinical coder, attention to detail is paramount. The role involves reviewing complex medical records and translating them into accurate codes. A single error in coding can have a significant impact on patient care, billing, and healthcare analytics. By developing a keen eye for detail, you will ensure the codes accurately reflect the medical documentation, enabling healthcare providers to deliver appropriate and effective care.
Analytical Thinking
Analytical thinking is another key skill for clinical coders. The ability to analyze medical records, determine the appropriate codes based on established guidelines, and identify any inconsistencies or missing information is essential. Moreover, clinical coders are often required to interpret complex medical procedures and diagnoses and translate them into coding language. Strong analytical skills will enable you to make informed decisions and ensure the accuracy and integrity of coded data.
Medical Terminology
Proficiency in medical terminology is fundamental to becoming a successful clinical coder. Understanding medical jargon, abbreviations, and the anatomical and physiological aspects of diseases and procedures is crucial for accurate coding. As a clinical coder, you will need to familiarize yourself with terms related to various specialties, such as cardiology, dermatology, or orthopedics. A solid foundation in medical terminology will facilitate your coding accuracy and efficiency.
Coding Systems Knowledge
a comprehensive knowledge of coding systems is a must for clinical coders. The most widely used coding systems in healthcare are the International Classification of Diseases (ICD) and the Current Procedural Terminology (CPT). Mastery of these systems is essential for correctly assigning diagnostic and procedural codes. Additionally, familiarity with other coding systems, such as Healthcare Common Procedure Coding System (HCPCS), will further expand your coding capabilities and make you a valuable asset to your employer.
Computer Skills
Clinical coding is a highly computerized field. Proficiency in computer skills is therefore essential for clinical coders. You will use specialized software and electronic health record systems (EHRs) to access patient records, assign codes, and generate reports. Moreover, you should be comfortable working with spreadsheets and databases, as this field involves managing and analyzing large volumes of data. Strong computer skills will enable you to work efficiently and stay up-to-date with the latest coding technologies.
Gaining Experience
This image is property of d3njjcbhbojbot.cloudfront.net.
Internships
Gaining practical experience through internships can be highly beneficial in your journey to becoming a clinical coder. Internships provide you with hands-on exposure to the healthcare environment, allowing you to apply your theoretical knowledge in a real-world setting. It is an opportunity to work closely with experienced coding professionals, learn from their expertise, and refine your coding skills. Internships can also serve as a gateway to potential job opportunities, as they often provide a foot in the door to the industry.
Volunteering
Volunteering at healthcare facilities, such as hospitals or clinics, can also provide valuable experience and networking opportunities. While volunteering may not directly involve coding tasks, it allows you to observe coding processes, interact with healthcare professionals, and gain insights into the healthcare industry. By dedicating your time and skills, you demonstrate your commitment to the field and build your professional network, potentially opening doors to future coding positions.
Entry-Level Positions
Securing entry-level positions in healthcare settings, such as medical coding clerk or coding assistant, can provide you with practical experience and further develop your coding skills. These positions often involve assisting experienced coders, reviewing medical records, and performing coding tasks under supervision. By immersing yourself in a coding environment, you will gain familiarity with coding procedures, coding software, and coding audits. Entry-level positions also provide an opportunity for continuous learning and growth as you work towards more advanced coding roles.
Getting Certified
Certification Importance
Obtaining certification in clinical coding is highly regarded within the healthcare industry. It demonstrates your proficiency and dedication to maintaining high coding standards. Many healthcare organizations and employers prioritize certified coders when hiring, as certifications validate your knowledge, skills, and adherence to coding guidelines. Certification enhances your credibility, expands your job prospects, and increases your earning potential as a clinical coder.
AHIMA Certification
The American Health Information Management Association (AHIMA) offers two primary certifications in clinical coding: the Certified Coding Associate (CCA) and the Certified Coding Specialist (CCS) credentials. The CCA certification is suitable for entry-level coding positions, while the CCS certification is geared towards more experienced coders. AHIMA certifications require passing a comprehensive exam that assesses your knowledge of medical coding guidelines, coding systems, and healthcare regulations.
AAPC Certification
The American Academy of Professional Coders (AAPC) also offers a range of certifications for clinical coders, including the Certified Professional Coder (CPC) and the Certified Outpatient Coder (COC) credentials. The CPC certification is widely recognized and is suitable for coders working in outpatient settings, such as physician offices or ambulatory surgery centers. The COC certification, on the other hand, focuses specifically on outpatient facility coding. AAPC certifications require passing a rigorous exam that tests your coding knowledge, industry guidelines, and proper use of coding systems.
Exam Preparation
Preparing for certification exams requires dedication and extensive study. There are numerous resources available, such as textbooks, online courses, and practice exams, that can help you prepare effectively. It is recommended to thoroughly review coding guidelines, brush up on medical terminology, and practice assigning codes to case studies. Additionally, attending exam preparation workshops or joining study groups can provide valuable insights and support from fellow coders. Adequate exam preparation will boost your confidence and increase your chances of passing the certification exam on your first attempt.
Continuing Education and Professional Development
This image is property of www.stepintothenhs.nhs.uk.
Continuing Education Units (CEUs)
Continuing education is crucial for clinical coders to stay updated with evolving coding practices, regulatory changes, and advancements in the healthcare industry. Many certifying organizations require coders to earn a certain number of Continuing Education Units (CEUs) to maintain their certification. CEUs can be obtained through various means, such as attending workshops, webinars, conferences, or completing online courses. By regularly participating in continuing education, you demonstrate your commitment to continuous learning and professional growth, ensuring you remain a competent and sought-after clinical coder.
Specialization and Advanced Certifications
As you gain experience and expertise in clinical coding, you may choose to specialize in specific areas of healthcare. Specialization can open up new opportunities and increase your marketability. Examples of specialized coding fields include cardiology, oncology, orthopedics, and pediatrics. Obtaining advanced certifications in these specialties, such as AHIMA’s Certified Coding Specialist-Physician-Based (CCS-P) credential or AAPC’s Certified Professional Medical Auditor (CPMA) certification, will further validate your knowledge and skills in your chosen specialization.
Workshops and Conferences
Attending workshops and conferences related to clinical coding provides valuable networking opportunities and allows you to stay abreast of industry trends and best practices. These events often feature expert speakers who share their insights and knowledge, helping you stay current in your coding profession. Workshops may focus on specific coding topics or provide hands-on coding practice, while conferences offer a broader perspective on healthcare industry developments. Participating in such events nurtures personal and professional growth, expands your network, and exposes you to new ideas and perspectives.
Job Search Strategies
Resume and Cover Letter
When searching for a clinical coding position, a well-crafted resume and cover letter are essential tools for showcasing your skills and qualifications. Tailor your resume to highlight your relevant education, certifications, and experience in medical coding. Include specific examples of your coding prowess, such as your accuracy rate and the coding systems you are proficient in. In your cover letter, emphasize your passion for accurate coding, attention to detail, and your ability to contribute effectively within a healthcare team. A polished and professional resume and cover letter will make you stand out among other candidates.
Networking
Networking is a powerful tool for job seekers, and it holds true for clinical coders as well. Attend professional events, join coding associations, and connect with peers and established coders in the field. Networking can open doors to hidden job opportunities, provide mentorship, and offer insights into the industry. Building relationships with professionals in healthcare administration, revenue cycle management, and other related fields can also expand your career possibilities beyond coding. Remember to maintain a professional online presence on platforms such as LinkedIn to enhance your networking efforts.
Online Job Boards
Online job boards specifically catering to healthcare and coding professions can be valuable resources for job seekers. These platforms often feature a wide range of coding positions, from entry-level to advanced roles. Regularly search and apply for relevant coding positions on reputable job boards, and make sure your resume and online profile are up to date. It is also recommended to explore industry-specific job boards and coding forums, as they may contain job opportunities that are not available on general job boards.
Professional Associations
Joining professional coding associations, such as AHIMA or AAPC, can provide numerous benefits for your job search. These associations often have job boards exclusively for members, offer career resources, and provide networking opportunities. Additionally, membership in professional associations demonstrates your commitment to the profession, enhances your professional credibility, and gives you access to industry news and updates. Participating actively in association activities, such as volunteering for committees or attending local chapter meetings, can also increase your visibility within the coding community.
Interview Preparation
This image is property of www.northwestcareercollege.edu.
Research the Company and Role
Before any interview, it is crucial to thoroughly research the prospective employer and the specific role you are applying for. Familiarize yourself with the organization’s mission, values, and services. Understand their coding processes, coding systems they use, and any coding-related initiatives they may have. This knowledge will allow you to tailor your interview responses to the organization’s specific needs and demonstrate your genuine interest in the position.
Prepare for Competency-based Questions
Many interviewers use competency-based or behavioral questions to assess candidates’ skills and experiences. Prepare for these types of questions by reflecting on your previous coding experiences and identifying specific examples that demonstrate your expertise. Practice answering questions that relate to attention to detail, analytical thinking, decision-making, and teamwork. Providing concrete examples of successful coding projects or challenges you have overcome will illustrate your competency and strengthen your chances of securing the position.
Highlight Relevant Experience
During the interview, make sure to highlight any relevant experience you have gained through internships, volunteering, or entry-level positions. Discuss how these experiences have prepared you for the challenges of clinical coding and emphasize any notable achievements or skills developed during these opportunities. By showcasing your hands-on experience and expertise, you will differentiate yourself from other candidates and demonstrate your readiness to contribute to the organization.
Ask Intelligent Questions
At the end of the interview, when given the opportunity, ask intelligent questions that demonstrate your knowledge of the industry and your commitment to the field. Inquire about the organization’s coding team, their training and development programs, mentoring opportunities, and any potential career growth pathways. Engaging the interviewer with thoughtful questions shows your enthusiasm and long-term commitment to the coding profession.
Starting Your Career
Entry-Level Positions
As a newly certified clinical coder, starting your career in an entry-level position is a common pathway. These positions often involve working in healthcare facilities, such as hospitals, clinics, or coding companies. During your initial years, focus on building a strong foundation in coding, gaining hands-on experience, and expanding your knowledge of various specialties. Embrace every learning opportunity and strive for continuous improvement, as this will set the stage for your future career growth.
Career Advancement Opportunities
Advancement opportunities in clinical coding can come in various forms. As you gain experience and demonstrate your skills, you may have the opportunity to take on more complex coding assignments or move into a senior coding role. Some clinical coders choose to pursue management positions, such as coding supervisors or coding managers, where they oversee coding teams and ensure coding compliance. Others may opt to specialize further in specific coding areas, becoming subject matter experts or consultants. Continuously seeking professional development and demonstrating your commitment to excellence will open the doors to a rewarding and diverse career path.
Specialization Pathways
As your career progresses, you may decide to specialize in a particular area of clinical coding. Specialization allows you to deepen your knowledge and expertise in specific medical specialties or coding systems. For example, you might choose to specialize in inpatient coding, outpatient coding, professional fee coding, or risk adjustment coding. By becoming a specialist in a particular area, you position yourself as a highly sought-after expert, potentially gaining access to more challenging coding assignments, increased compensation, and career advancement opportunities.
Job Prospects and Salary
Growing Demand for Clinical Coders
The demand for skilled and certified clinical coders continues to grow in the ever-evolving healthcare industry. As healthcare organizations strive to improve coding accuracy, data integrity, and compliance, the need for competent clinical coders becomes paramount. The increasing reliance on coding data for healthcare analytics, research, and reimbursement further contributes to the demand for qualified coders. By pursuing a career in clinical coding, you are entering a profession with promising job prospects and excellent opportunities for growth and advancement.
Salary Range
The salary range for clinical coders can vary depending on factors such as location, experience, education, and certifications. Entry-level positions typically offer lower salaries, as they serve as a starting point for gaining experience and advancing in the field. As you gain experience and expertise, your earning potential as a clinical coder increases. According to national salary data, the average annual salary for clinical coders ranges from $45,000 to $70,000 USD. Advanced certifications, specialization, and management roles often command higher salaries within the field.
Factors Affecting Salary
Several factors can influence the salary of a clinical coder. Firstly, geographic location plays a significant role, as salaries tend to vary depending on the cost of living and regional demand for coders. Urban areas often have a higher demand for coders and may offer higher salaries compared to rural areas. Secondly, the level of experience and education also affects salary levels. Clinical coders with advanced degrees, certifications, and several years of experience typically command higher salaries. Lastly, working in specialized areas, such as risk adjustment coding or auditing, can lead to higher salary levels due to the specialized knowledge and skills required.
Challenges and Rewards
Dealing with Complexity
Clinical coding is a complex and detail-oriented field that presents its fair share of challenges. Interpreting and translating intricate medical documentation into accurate codes can be demanding, especially when faced with ambiguous or incomplete information. Clinical coders must continuously update their knowledge of coding guidelines and keep up with ever-changing healthcare regulations. Despite the challenges, the complexity of clinical coding provides continuous intellectual stimulation and growth opportunities for individuals who thrive in a challenge-driven environment.
Contributing to Healthcare System
One of the most rewarding aspects of a career in clinical coding is the direct impact on the healthcare system. Accurate coding ensures that healthcare providers are appropriately reimbursed for their services, which, in turn, contributes to the financial sustainability of healthcare organizations. By assigning correct codes, clinical coders facilitate accurate research, quality improvement efforts, and epidemiological studies. They play a vital role in healthcare analytics, tracking disease patterns, and identifying areas for improvement in patient care. Clinical coders are the backbone of healthcare data management and contribute significantly to the overall effectiveness and efficiency of the healthcare industry.
Continuous Learning and Professional Growth
Clinical coding is a profession that fosters continuous learning and professional growth. The ever-evolving nature of healthcare necessitates staying updated on coding guidelines, regulatory changes, and advancements in technology. As you progress in your career, pursuing advanced certifications, attending conferences, and participating in continuing education programs will allow you to expand your knowledge and remain a valuable asset to your employer. The professional growth opportunities in clinical coding are vast, ranging from advanced coding roles and management positions to specialized coding fields and consulting opportunities.
In conclusion, becoming a clinical coder requires a solid educational foundation, specialized training, and certifications. Attention to detail, analytical thinking, medical terminology, coding systems knowledge, and computer skills are essential qualities for success in this field. Gaining practical experience through internships, volunteering, and entry-level positions is crucial for career development. Obtaining certifications from reputable organizations like AHIMA and AAPC demonstrates your competence and dedication to the field. Continuing education, specialization, and active involvement in professional associations are vital for professional growth. Job search strategies, interview preparation, and a strong start in entry-level positions pave the way for a successful career. Clinical coding offers promising job prospects, a range of salary options, and opportunities for continuous learning and professional growth. Overcoming the challenges, contributing to the healthcare system, and embracing the rewards make clinical coding a fulfilling and rewarding profession.
In the realm of healthcare administration, understanding the intricacies of the medical billing process is crucial. With the ever-increasing complexity of medical billing codes and regulations, it is essential to have a clear grasp of the sequential steps involved. This article aims to provide a concise overview of the 10 fundamental steps in the medical billing process, allowing you to navigate this intricate terrain with confidence and proficiency.
Pre-Registration
Gathering patient information
The first step in the medical billing process is pre-registration, which involves gathering important patient information. This information includes the patient’s name, date of birth, contact details, and insurance information. It is crucial to collect accurate and up-to-date information to ensure smooth billing and claims processing.
Verifying insurance eligibility
After collecting patient information, the next step is to verify insurance eligibility. This involves contacting the insurance company to check if the patient’s policy is active and to determine the coverage and benefits. Verifying insurance eligibility enables healthcare providers to understand the patient’s insurance coverage and make informed decisions regarding treatment and billing.
Scheduling appointments
The final step in the pre-registration process is scheduling appointments for patients. This ensures that patients have a designated time to visit the healthcare facility for their medical services. Scheduling appointments aids in managing patient flow and ensures that medical professionals can provide timely and efficient care.
Check-in
Updating patient information
During the check-in process, patients are required to update their personal and insurance information. This step is crucial to ensure that the information on file is accurate and up to date. Patients may have changed their address, contact details, or insurance providers, and updating this information ensures that the billing process is accurate and efficient.
Collecting co-payments
The check-in process also involves collecting co-payments from patients. Co-payments are a portion of the medical costs that the patient is responsible for. Collecting co-payments upfront ensures that the patient has made their financial contribution towards their medical services and also helps in managing revenue for the healthcare facility.
Verifying insurance information
Verifying insurance information during check-in allows the healthcare facility to ensure that the insurance details provided by the patient are accurate and up to date. This step is important to avoid any potential issues with claims submission or denials due to incorrect insurance information. Verifying insurance information helps to streamline the billing process and ensure accurate reimbursement.
Coding
Assigning appropriate medical codes
Coding is a fundamental step in the medical billing process, where healthcare professionals assign specific medical codes to diagnoses, procedures, and services provided during a patient’s visit. These codes help in accurately describing the patient’s medical condition and the services rendered. Assigning appropriate medical codes ensures proper reimbursement and adherence to coding guidelines.
Using diagnosis codes
Diagnosis codes, also known as International Classification of Diseases (ICD) codes, are used to describe the patient’s medical condition or illness. These codes provide detailed information about the diagnosis, which helps in proper billing and claims submission. Using accurate diagnosis codes ensures that claims are processed smoothly and reflects the patient’s medical needs accurately.
Using procedure codes
Procedure codes, also known as Current Procedural Terminology (CPT) codes, are used to describe the specific medical procedures or services provided to the patient. These codes provide information about the type of service, the complexity, and the resources involved in delivering the care. Using procedure codes assists in accurate billing and enables appropriate reimbursement for the healthcare services provided.
Charge Entry
Medical cost concept with stethoscope and medical bill
Recording charges for services rendered
Charge entry involves recording the charges for the services rendered to patients. This step includes documenting the specific procedures, tests, or treatments provided during the patient’s visit. Accurate charge entry is vital as it ensures that the healthcare facility is appropriately reimbursed for the services provided and reflects the value of the care delivered.
Verifying charges for accuracy
Before entering charges into the billing system, it is essential to verify their accuracy. This involves reviewing the documentation, medical codes, and the fee schedule to ensure that the charges align with the services provided. Verifying charges for accuracy minimizes errors, reduces potential billing disputes, and ensures that the billing process is transparent and compliant.
Entering charges into the billing system
After verifying the charges, the next step is to enter them into the billing system. This involves inputting the relevant information, such as the medical codes, patient details, and any required modifiers, into the billing software or electronic health record system. Entering charges into the billing system paves the way for claims submission and further processing.
Claim Submission
Generating and reviewing claim forms
Claim submission is a critical step in the medical billing process, where healthcare providers generate and review claim forms. These forms contain all the necessary information, including the patient’s demographics, insurance details, medical codes, and any supporting documentation. Generating and reviewing claim forms ensures completeness and accuracy before submission to the insurance company.
Attaching necessary documentation
Along with claim forms, it may be necessary to attach additional documentation that supports the services provided or justifies medical necessity. This can include progress notes, test results, or referral documents from other healthcare providers. Attaching necessary documentation provides comprehensive information to the insurance company, increasing the chances of successful claim processing.
Submitting claims to insurance companies
Once the claim forms and supporting documentation are prepared, they are submitted to the appropriate insurance companies for processing. This step involves sending the claims electronically or via mail, depending on the insurance provider’s requirements. Submitting claims in a timely manner ensures prompt reimbursement and minimizes delays in the billing process.
Insurance Verification
Verifying insurance coverage and benefits
Insurance verification is a crucial step in the medical billing process, where healthcare providers confirm the patient’s insurance coverage and benefits. This involves contacting the insurance company to verify the policy details, including deductibles, co-insurance, and coverage limits. Verifying insurance coverage and benefits helps in estimating the patient’s financial responsibility and aids in accurate billing.
Confirming patient and provider information
In addition to insurance coverage, it is essential to confirm the accuracy of patient and provider information during insurance verification. This ensures that the correct patient and provider details are included in the claim submission. Confirming patient and provider information avoids potential claim rejections or delays due to incorrect or mismatched information.
Determining pre-authorization requirements
Certain healthcare services or procedures may require pre-authorization from the insurance company before they can be performed. Insurance verification helps in determining these pre-authorization requirements. This involves checking if medical services require prior approval and following the necessary steps to obtain the authorization. Understanding pre-authorization requirements helps in avoiding claim denials and ensuring reimbursement.
Claim Processing
Reviewing claims for completeness and accuracy
After the insurance company receives the claims, they are reviewed for completeness and accuracy. This involves checking if all the necessary information, including medical codes, documentation, and patient details, is present. Reviewing claims for completeness and accuracy helps in minimizing claim rejections and ensures that the claims are processed effectively.
Adjudicating claims based on insurance policies
Claim adjudication is the process where the insurance company reviews the submitted claims and makes decisions regarding coverage and payment. This step involves comparing the services provided with the policy’s benefits and coverage limitations. Adjudicating claims based on insurance policies determines the amount that will be reimbursed to the healthcare provider.
Applying payment adjustments or denials
During claim processing, the insurance company may apply payment adjustments or denials based on their policies and coverage limitations. Payment adjustments can include deductibles, co-pays, or contractual obligations with the healthcare provider. Denials occur when the insurance company determines that the services provided are not covered or do not meet medical necessity. Applying payment adjustments or denials concludes the claim processing stage.
Payment Posting
Recording payments received from insurance companies
Payment posting involves recording the payments received from insurance companies for the services rendered. This step includes updating the patient’s account and reflecting the insurance company’s reimbursement in the financial records. Recording payments received from insurance companies ensures accurate tracking of payments and helps in managing accounts receivable.
Applying payments to patient accounts
Once the payments are recorded, they are then applied to the respective patient accounts. This involves reconciling the payment with the outstanding balances and adjusting the account accordingly. Applying payments to patient accounts ensures that the correct balance is reflected and facilitates accurate financial reporting.
Notifying patients of outstanding balances
In cases where the insurance company’s payment does not cover the full amount due, there may be an outstanding balance remaining for the patient to pay. Notifying patients of outstanding balances is essential to prompt them to settle their financial responsibility. This step involves generating patient statements and providing detailed explanations of the charges and payments received.
Denial Management
Identifying and resolving claim denials
Denial management is an important aspect of the medical billing process. It involves identifying the reasons for claim denials and taking appropriate action to resolve them. This may include reviewing the denial reason, correcting coding or documentation errors, and resubmitting the claim for reconsideration. Identifying and resolving claim denials ensures maximum reimbursement for the services provided.
Appealing denied claims if necessary
If claim denials cannot be resolved through regular channels, healthcare providers have the option to appeal the decision. Appealing denied claims involves presenting additional documentation, evidence, or justification for the medical necessity of the services provided. Appealing denied claims allows healthcare providers to advocate for proper reimbursement and challenge unfavorable decisions.
Updating coding or documentation as needed
As part of denial management, updating coding or documentation may be necessary to address the reasons for claim denials. This can involve reviewing the medical codes used, modifying the diagnosis or procedure codes, or improving the supporting documentation. Updating coding or documentation addresses any deficiencies and helps in successfully resubmitting the claim for reimbursement.
Patient Billing and Follow-up
Generating patient statements
Patient billing is the final step in the medical billing process, where healthcare providers generate and send statements to patients for their outstanding balances. Generating patient statements includes consolidating all the charges, payments, and adjustments into a single document that clearly outlines the financial responsibility. Patient statements provide transparency and facilitate prompt payment collection.
Providing detailed explanation of charges
Along with patient statements, it is important to provide patients with a detailed explanation of the charges incurred. This may involve itemizing the services provided, showcasing the corresponding medical codes, and offering a breakdown of any insurance adjustments or payments. Providing a detailed explanation of charges ensures that patients understand the billing process and can address any questions or concerns.
Following up on unpaid balances
Following up on unpaid balances is crucial for efficient revenue management. This involves contacting patients who have outstanding balances, sending reminders, and working with them to arrange payment plans or resolve any billing discrepancies. Following up on unpaid balances ensures timely collection of payments and helps maintain positive patient-provider relationships.
In conclusion, the medical billing process consists of various interconnected steps that require attention to detail, accurate information gathering, and adherence to coding and insurance guidelines. From pre-registration to patient billing and follow-up, each step plays a vital role in ensuring smooth and accurate billing, appropriate reimbursement, and maintaining financial stability for healthcare providers. By following these ten steps diligently, healthcare facilities can streamline their billing processes and provide optimal patient care.
In the complex landscape of medical billing, denials are an ever-present challenge for healthcare providers. Understanding the various types of denials is crucial for both medical billing professionals and healthcare organizations alike. From insurance policy exclusions to coding errors and eligibility issues, this article explores the common types of denials in medical billing, shedding light on how they impact revenue cycles and tips for preventing and resolving them efficiently.
Claim Denials
This image is property of nemadji.org.
Authorization Denials
Authorization denials occur when a healthcare provider fails to obtain proper authorization from the insurance company before providing services or procedures to a patient. Insurance companies require authorization to ensure that the treatment or service is medically necessary and meets their coverage criteria. Without proper authorization, the insurance company may deny the claim, leaving the provider to bear the financial burden.
To avoid authorization denials, providers should familiarize themselves with each insurance company’s specific requirements for authorization. They should also ensure that all necessary documentation, such as medical records or supporting documents, is submitted with the authorization request. Clear communication between the provider and the insurance company is crucial to avoid any misunderstandings or delays in obtaining authorization.
Eligibility Denials
Eligibility denials occur when a healthcare provider submits a claim for a patient who is not covered under the patient’s insurance policy or whose coverage has expired. Insurance companies maintain databases that contain information on each individual’s insurance coverage, including eligibility status. Providers should verify a patient’s eligibility and coverage before rendering any services to avoid eligibility denials.
To prevent eligibility denials, providers can implement a robust verification process. This process involves verifying a patient’s insurance coverage, confirming the effective dates of the policy, and checking for any exclusions or limitations that may affect coverage. Accurate and up-to-date patient information, such as insurance ID numbers and demographic details, is essential for a successful eligibility verification process.
Technical Denials
Technical denials occur due to errors or issues related to the technical aspects of claim submission. These denials are often the result of incomplete or incorrect information provided on the claim form, such as missing or invalid codes, incorrect patient information, or formatting errors. Insurance companies have specific guidelines and requirements for claim submission, and failing to adhere to these guidelines can result in a technical denial.
To avoid technical denials, providers should invest in robust claims management software or systems that can help validate claims before submission. These systems can check for errors and inconsistencies, ensuring that all required fields are completed accurately. Providers should also regularly train their billing staff to stay updated on the latest claim submission guidelines and requirements.
Medical Necessity Denials
Medical necessity denials occur when a service or procedure rendered to a patient is deemed not medically necessary by the insurance company. Insurance companies use medical guidelines and criteria to determine what they consider medically necessary. If a service or procedure does not meet these criteria, the insurance company may deny the claim, leaving the provider responsible for the charges.
To prevent medical necessity denials, providers should thoroughly document the patient’s medical condition and the need for the service or procedure. It is crucial to provide clear and concise documentation that supports the medical necessity of the claim. Providers should also familiarize themselves with the medical policies and guidelines of the insurance companies they work with to ensure that the services they provide align with the insurers’ criteria.
Duplicate Claim Denials
Duplicate claim denials occur when a provider submits multiple claims for the same service or procedure, resulting in duplicate charges. Insurance companies have systems in place to detect and reject duplicate claims to prevent overbilling. Providers should ensure that they have proper checks and balances in place to prevent duplicate claim submissions. Regular audits of claim submissions can help identify any potential duplicates and rectify the issue before the claim is denied.
To prevent duplicate claim denials, providers should employ effective billing and claims management systems that can detect and prevent duplicate submissions. Clear communication within the billing department is essential to avoid inadvertent duplicate submissions. Well-documented procedures and protocols for claim submission can also help prevent errors that may lead to duplicate claims.
Timely Filing Denials
Timely filing denials occur when a provider fails to submit a claim within the designated timeframe specified by the insurance company. Insurance companies typically have strict guidelines regarding the submission of claims, and failure to comply with these guidelines can result in a denial. Each insurance company may have varying deadlines for claim submission, making it crucial for providers to stay informed about these deadlines.
To avoid timely filing denials, providers should establish efficient and well-organized billing processes that prioritize timely claim submission. Clear communication between the billing department and the healthcare providers is essential to ensure that all necessary documentation and codes are collected in a timely manner. Regular monitoring and tracking of claim submissions can help identify any potential delays and address them promptly.
Coordination of Benefits Denials
Coordination of benefits denials occur when a patient has multiple insurance coverages, and the primary and secondary insurance companies do not coordinate their coverage properly. This type of denial often arises due to errors in updating insurance information or lack of clear communication between the patient, provider, and insurance companies. Providers must ensure that accurate and up-to-date insurance information is obtained from the patient and that all relevant insurance companies are properly notified.
To prevent coordination of benefits denials, providers should have a clear understanding of the patient’s insurance coverage and coordination of benefits requirements. Verification of insurance information should be conducted at each visit to ensure accurate billing. Establishing effective communication channels with patients and insurance companies can help minimize errors and prevent coordination of benefits denials.
Non-Covered Service Denials
Non-covered service denials occur when a service or procedure rendered to a patient is not covered under the patient’s insurance policy. Insurance companies have specific coverage policies that outline what services, procedures, or treatments they consider covered. Providers should verify the patient’s coverage and eligibility for specific services before rendering them.
To prevent non-covered service denials, providers should have a clear understanding of the insurance policies they work with and their coverage criteria. Clear communication with the patient is essential to ensure that they understand what services are covered under their insurance policy and what may be considered non-covered. When there is uncertainty regarding coverage, obtaining a predetermination or prior authorization from the insurance company can help clarify any potential coverage issues.
Coding Denials
Coding denials occur when there are errors or inconsistencies in the codes used on the claim form. Common coding errors include using incorrect procedure codes, diagnosis codes, or modifiers. Insurance companies rely heavily on these codes to determine coverage and reimbursement, and discrepancies or errors can result in denials.
To prevent coding denials, providers should invest in regular training and education for their coding staff to ensure they are up to date with the latest coding guidelines and changes. The use of comprehensive coding manuals and coding software can also help minimize coding errors. Regular audits of coding practices can assist in identifying any areas of improvement and reducing coding-related denials.
Reimbursement Denials
Reimbursement denials occur when an insurance company denies payment for a service or procedure despite the claim meeting all necessary requirements. This type of denial can be frustrating for providers as they have provided the service or procedure but are not appropriately reimbursed. Reimbursement denials can occur due to various reasons, including errors in claim processing, fee schedule limitations, or lack of coverage for a specific service.
To address reimbursement denials, providers should conduct thorough reviews of the denial reasons and processes. Identifying patterns or common issues can help tailor solutions to reduce future denials. Effective communication with the insurance company, appeals processes, and detailed documentation of services rendered can potentially resolve reimbursement denials.
Payment Denials
Partial Payment Denials
Partial payment denials occur when an insurance company approves the claim but reimburses the provider with only a portion of the billed amount. This typically happens when the insurance company applies contractual adjustments, such as negotiated rates or fee schedules, which reduce the payment amount. Providers should familiarize themselves with the reimbursement rates for each insurance company to manage their revenue expectations accurately.
To mitigate partial payment denials, providers can consider negotiating favorable contracts with insurance companies. They can also implement sound financial policies that include clear communication to patients about their financial responsibilities, such as co-pays or deductibles. By managing patient expectations and setting up clear payment guidelines, providers can minimize potential partial payment denials.
Full Payment Denials
Full payment denials occur when an insurance company denies payment for the entire claim, leaving the provider with no reimbursement. This can happen due to various reasons, such as lack of coverage for the service, billing errors, or failure to meet specific claim submission requirements. Providers should thoroughly review the denial reasons and follow the necessary steps to address the issue promptly.
To address full payment denials, providers should review their claim submission processes and ensure compliance with insurance company requirements. Verifying patient coverage, accurate coding, and proper documentation are vital to preventing full payment denials. Prompt and thorough appeals, along with effective communication with the insurance company, can increase the chances of successful resolution.
Downcoding Denials
Downcoding denials occur when an insurance company reduces the level of service or downcodes the claim, resulting in lower reimbursement. This often happens when the documentation does not support the level of service billed by the provider. Providers must ensure that their documentation accurately reflects the complexity and severity of the patient’s condition to avoid downcoding denials.
To prevent downcoding denials, providers should implement robust documentation practices that capture the level of service accurately. Clear and detailed documentation should include the patient’s medical history, examination findings, and the rationale for the services provided. Regular auditing of documentation and coding practices can help identify any potential downcoding issues and address them promptly.
Bundled Payment Denials
Bundled payment denials occur when an insurance company groups multiple services or procedures into a single reimbursement, resulting in a lower payment than expected. This typically happens when the insurance company has specific bundling rules in place, and the services provided by the provider are considered bundled under those rules. Providers should be aware of the bundling rules of each insurance company to accurately bill for their services.
To prevent bundled payment denials, providers should familiarize themselves with the bundling rules and guidelines of the insurance companies they work with. Ensuring that the services provided are appropriately billed and documented can minimize the risk of bundled payment denials. In cases where bundling is necessary, providers should clearly communicate with the patient and insurance company to manage expectations.
Rejection Denials
Rejection denials occur when the insurance company rejects a claim due to errors or inconsistencies in the claim submission process. Unlike denials, rejections refer to claims that are not even considered for payment due to issues that can be resolved by fixing the errors and resubmitting the claim. Providers should review rejection reasons and promptly address the issues to ensure timely payment.
To prevent rejection denials, providers should implement robust claim scrubbing processes that can identify and correct errors before submission. Verification of patient and insurance information, accurate coding, and thorough documentation are essential to prevent rejections. Regular monitoring and tracking of claim submissions can help identify any potential issues and rectify them promptly.
Appeal Denials
Administrative Denials
Administrative denials occur when a claim is denied due to administrative errors or omissions in the claim submission process. These errors can include missing or incomplete information, such as provider identification numbers, patient demographics, or authorization details. Providers should thoroughly review denial reasons and address any administrative issues promptly.
To address administrative denials, providers should establish clear protocols and procedures for claim submission that cover all necessary administrative requirements. Regular staff training and education on claim submission guidelines can help minimize administrative errors. Thorough reviews of claim documentation before submission can also help identify any missing or incomplete information and rectify it promptly.
Corrected Claim Denials
Corrected claim denials occur when a corrected or updated claim is denied after the initial claim was denied. This can happen if the corrections made to the claim do not address the reasons for denial or if the necessary documentation is not provided to support the corrections. Providers should carefully review denial reasons and ensure that all necessary information is included in the corrected claim.
To prevent corrected claim denials, providers should thoroughly review the original denial reasons and address them adequately. Clear documentation of the corrections made, along with any supporting documentation, should be included with the corrected claim. Regular communication with the insurance company and timely follow-up can help ensure that the corrected claim is processed without further denials.
Medical Record Denials
Medical record denials occur when the insurance company requests additional medical records or documentation to support a claim, and the provider either fails to provide the requested records or the records are incomplete or insufficient. Insurance companies rely on medical records to determine the validity and medical necessity of the services provided, and the lack of proper documentation can lead to claim denials.
To prevent medical record denials, providers should establish clear processes for medical record requests and ensure that all necessary documentation is provided promptly. Regular reviews of medical record documentation and audits can help identify any potential gaps or deficiencies in the documentation. Effective communication with the billing and medical staff is crucial to ensure that the requested records are provided promptly and accurately.
Medical Necessity Denials
Medical necessity denials in the appeal process occur when an insurance company continues to deny a claim based on their judgement that the service or procedure is not medically necessary, despite the provider’s appeal. This can happen when there is a difference of opinion between the provider and the insurance company regarding the need and appropriateness of the services provided. Providers should be prepared to provide clear and convincing documentation that supports the medical necessity of the services to overturn such denials.
To address medical necessity denials in the appeal process, providers should ensure that their appeal includes comprehensive and well-documented medical records that clearly articulate the patient’s condition and the need for the services provided. Engaging with the insurance company to understand their specific criteria and guidelines for medical necessity can help tailor the appeal and strengthen the documentation provided. Prompt follow-up and persistence in the appeal process can sometimes lead to a successful resolution.
Timely Filing Denials
Timely filing denials in the appeal process occur when the provider submits an appeal beyond the designated timeframe specified by the insurance company. Insurance companies often have strict deadlines for appeals, and failing to adhere to these deadlines can result in denials. Providers should familiarize themselves with the appeal deadlines of each insurance company to ensure timely submission.
To prevent timely filing denials in the appeal process, providers should establish efficient and well-organized appeal processes that prioritize timely submission. Clear communication between the billing department, the healthcare providers, and any necessary external resources, such as legal counsel or consultants, is essential to ensure that all necessary documentation and codes are collected in a timely manner. Regular monitoring and tracking of appeal submissions can help identify any potential delays and address them promptly.
Billing Denials
Medical cost concept with stethoscope and medical bill
Incorrect Patient Information Denials
Incorrect patient information denials occur when patient information, such as name, date of birth, or insurance information, is entered inaccurately or incompletely on the claim form. Insurance companies rely on accurate patient information for claim processing, and discrepancies or errors can result in denials. Providers should ensure that they obtain and verify accurate patient information for each claim submission.
To prevent incorrect patient information denials, providers should implement robust patient registration and verification processes that capture accurate patient information. Regular staff training and education on the importance of accurate patient information can help minimize errors. Verification of patient demographics and insurance information at each visit can help ensure that accurate information is collected for claim submission.
Incorrect Provider Information Denials
Incorrect provider information denials occur when the provider’s information, such as identification numbers or credentials, is entered inaccurately or incompletely on the claim form. Insurance companies rely on accurate provider information for claim processing, and errors or discrepancies can result in denials. Providers should ensure that their information is accurately updated and communicated to the insurance company.
To prevent incorrect provider information denials, providers should regularly update and verify their provider information with the insurance companies they work with. Clear communication channels should be established to notify insurance companies of any changes or updates to the provider’s information. Regular reviews of claim submissions can help identify any potential errors or inconsistencies in the provider information and rectify them promptly.
Non-Compliance Denials
Non-compliance denials occur when a provider fails to comply with specific regulatory or contractual requirements set by the insurance company. These requirements can include timely submission of claims, adherence to coding and billing guidelines, or participation in specific programs or networks. Providers should thoroughly review their contracts and agreements with insurance companies to ensure compliance with all requirements.
To prevent non-compliance denials, providers should familiarize themselves with the specific requirements of each insurance company they work with. Establishing clear protocols and procedures that prioritize compliance with regulatory and contractual requirements can help minimize non-compliance denials. Regular reviews of billing and coding practices, as well as internal audits, can help identify any potential non-compliance issues and rectify them promptly.
Lack of Documentation Denials
Lack of documentation denials occur when there is insufficient or incomplete documentation to support the services or procedures billed on the claim form. Insurance companies rely on accurate and comprehensive medical records to determine the validity and medical necessity of the services provided. Insufficient documentation can result in denials, leaving the provider responsible for the charges.
To prevent lack of documentation denials, providers should implement robust documentation practices that capture all necessary information to support the services provided. Clear and detailed documentation should include the patient’s medical history, examination findings, treatment plans, and the rationale for the services provided. Regular training and education for medical and billing staff on documentation requirements can help minimize deficiencies in documentation.
Upcoding Denials
Upcoding denials occur when a provider submits a claim using codes that represent a higher level of service than what was actually provided. This can be an intentional or unintentional error and can result in increased reimbursement. Upcoding is considered fraudulent and can lead to severe consequences, including legal and financial penalties. Providers must ensure that their coding accurately reflects the services provided.
To prevent upcoding denials, providers should invest in regular training and education for their coding staff to ensure accurate coding practices. The use of comprehensive coding manuals and coding software can also help minimize upcoding errors. Regular audits of coding practices can assist in identifying any potential upcoding issues and address them promptly.
Unbundling Denials
Unbundling denials occur when a provider bills for separate services or procedures that should be billed together under a single code. Insurance companies have specific guidelines for bundling services, and failing to adhere to these guidelines can result in denials. Providers must ensure that their billing practices reflect accurate bundling of services.
To prevent unbundling denials, providers should familiarize themselves with the bundling rules and guidelines of the insurance companies they work with. It is essential to accurately code and bill for services based on the bundling rules, ensuring that services that should be bundled are not billed and charged separately. Regular reviews of billing practices and audits can help identify any potential unbundling issues and rectify them promptly.
Insurance Limit Denials
Insurance limit denials occur when a patient’s insurance coverage has reached its limit or maximum benefit for a specific service or procedure. Insurance policies often have limits on coverage amounts, such as annual maximums or visit limits for certain services. Providers should verify the patient’s coverage and ensure that the services provided are within the allowed limits to avoid insurance limit denials.
To prevent insurance limit denials, providers should verify the patient’s insurance coverage and limits before rendering services. This includes understanding any restrictions, maximums, or limitations set by the insurance company. Clear communication with the patient about their coverage and financial responsibilities is essential to manage expectations and minimize insurance limit denials.
Duplicate Billing Denials
Duplicate billing denials occur when a provider submits multiple claims for the same service or procedure, resulting in duplicate charges. Insurance companies have systems in place to detect and reject duplicate claims to prevent overbilling. Providers should ensure that they have proper checks and balances in place to prevent duplicate billing. Regular audits of billing practices can help identify any potential duplicates and rectify the issue before the claim is denied.
To prevent duplicate billing denials, providers should implement effective billing and claims management systems that can detect and prevent duplicate submissions. Clear communication within the billing department is essential to avoid inadvertent duplicate submissions. Well-documented procedures and protocols for billing can also help prevent errors that may lead to duplicate billing denials.
Service Not Authorized Denials
Service not authorized denials occur when a claim is denied because the insurance company did not authorize or approve the service or procedure. Providers must obtain proper authorization or pre-authorization from the insurance company before rendering the service to avoid service not authorized denials. Failure to obtain authorization can leave the provider responsible for the charges.
To prevent service not authorized denials, providers should familiarize themselves with each insurance company’s specific authorization requirements. They should also ensure that all necessary documentation, such as medical records or supporting documents, is submitted with the authorization request. Clear communication between the provider and the insurance company is crucial to avoid any misunderstandings or delays in obtaining authorization.
Expired Time Limit Denials
Expired time limit denials occur when a claim is denied due to submission beyond the designated timeframe specified by the insurance company. Insurance companies typically have strict guidelines regarding the submission of claims, and failure to comply with these guidelines can result in denials. Providers should familiarize themselves with the claim submission deadlines of each insurance company to ensure timely submission.
To prevent expired time limit denials, providers should establish efficient and well-organized billing processes that prioritize timely claim submission. Clear communication between the billing department and the healthcare providers is essential to ensure that all necessary documentation and codes are collected in a timely manner. Regular monitoring and tracking of claim submissions can help identify any potential delays and address them promptly.
Internal Denials
Coding Errors Denials
Coding errors denials occur when there are errors or inconsistencies in the codes used on the claim form within the provider’s own coding processes. These errors can result from incorrect coding practices, lack of training, or underutilization of coding resources. Providers must ensure that their coding practices follow the industry-standard guidelines and accurately reflect the services provided.
To prevent coding errors denials, providers should invest in regular training and education for their coding staff to ensure accurate coding practices. The use of comprehensive coding manuals and coding software can also help minimize coding errors. Regular audits of coding practices can assist in identifying any potential errors and provide opportunities for education and improvement.
Lack of Documentation Denials
Lack of documentation denials within the provider’s organization occur when there is insufficient or incomplete documentation to support the services or procedures billed on the claim form. Providers rely on accurate and comprehensive medical records to determine the validity and medical necessity of the services provided. Insufficient documentation can result in internal denials, creating financial losses for the organization.
To prevent lack of documentation denials within the provider’s organization, providers should implement robust documentation practices that ensure all necessary information to support the services provided is recorded accurately. Clear and detailed documentation should include the patient’s medical history, examination findings, treatment plans, and the rationale for the services provided. Regular training and education for medical and billing staff on documentation requirements can help minimize deficiencies in documentation.
Miscommunication Denials
Miscommunication denials occur when there is a breakdown in communication between different departments or individuals within the provider’s organization, leading to errors or inconsistencies in claim submission or billing processes. Clear and effective communication is vital to ensure accurate and timely claim processing. Regular staff meetings and collaboration can help minimize miscommunication denials.
To prevent miscommunication denials, providers should establish clear lines of communication and protocols for interdepartmental collaboration and information sharing. Regular staff meetings, training sessions, and updates on billing and claims processes can help ensure that everyone involved in the claims management process is on the same page. Clear escalation protocols and designated points of contact can help address and resolve any miscommunication issues promptly.
Incomplete Claim Denials
Incomplete claim denials occur when a claim is denied due to missing or incomplete information on the claim form within the provider’s organization. Insurance companies have specific guidelines and requirements for claim submission, and failure to adhere to these guidelines can result in denials. Providers should thoroughly review claim submission processes and ensure compliance with the insurance company’s requirements.
To prevent incomplete claim denials within the provider’s organization, providers should establish clear protocols and procedures for claim submission that cover all necessary requirements. Regular staff training and education on claim submission guidelines can help minimize errors. Thorough reviews of claim documentation before submission can also help identify any missing or incomplete information and rectify it promptly.
Coordination of Benefits Denials
Coordination of benefits denials within the provider’s organization occur when there is a failure to properly coordinate benefits for patients with multiple insurance coverages. This can be a result of errors in updating patient insurance information or a lack of clear communication between the patient, provider, and insurance companies. Providers must ensure that accurate and up-to-date insurance information is obtained from the patient and that all relevant insurance companies are properly notified.
To prevent coordination of benefits denials within the provider’s organization, providers should have a clear understanding of the patient’s insurance coverage and coordination of benefits requirements. Verification of insurance information should be conducted at each visit to ensure accurate billing. Establishing effective communication channels with patients and insurance companies can help minimize errors and prevent coordination of benefits denials.
External Denials
Inadequate Insurance Coverage Denials
Inadequate insurance coverage denials occur when a patient’s insurance policy does not provide sufficient coverage for the services rendered by the provider. This can include limitations on specific services or procedures, low coverage limits, or exclusions for certain types of treatments or conditions. Providers should verify the patient’s insurance coverage and ensure that the services provided are within the covered benefits.
To prevent inadequate insurance coverage denials, providers should thoroughly review the patient’s insurance policy and coverage before rendering services. Clear communication with the patient about their insurance coverage and financial responsibilities is essential to manage expectations and minimize inadequate coverage denials. In cases where there is uncertainty regarding coverage, obtaining a pre-authorization or predetermination from the insurance company can help clarify any potential coverage issues.
Authorization Denials
Authorization denials occur when a provider submits a claim for services or procedures that require prior authorization, but the insurance company denies the authorization request. Verification of authorization requirements and obtaining proper authorization from the insurance company before rendering services is crucial to avoid authorization denials. Failure to obtain authorization can leave the provider responsible for the charges.
To prevent authorization denials, providers should familiarize themselves with each insurance company’s specific requirements for authorization. They should also ensure that all necessary documentation, such as medical records or supporting documents, is submitted with the authorization request. Clear communication between the provider and the insurance company is crucial to avoid any misunderstandings or delays in obtaining authorization.
Medical Necessity Denials
Medical necessity denials occur when a service or procedure rendered to a patient is deemed not medically necessary by the insurance company. Insurance companies use medical guidelines and criteria to determine what they consider medically necessary. If a service or procedure does not meet these criteria, the insurance company may deny the claim, leaving the provider responsible for the charges.
To prevent medical necessity denials, providers should thoroughly document the patient’s medical condition and the need for the service or procedure. It is crucial to provide clear and concise documentation that supports the medical necessity of the claim. Providers should also familiarize themselves with the medical policies and guidelines of the insurance companies they work with to ensure that the services they provide align with the insurers’ criteria.
Incorrect Patient Information Denials
Incorrect patient information denials occur when patient information, such as name, date of birth, or insurance information, is entered inaccurately or incompletely on the claim form. Insurance companies rely on accurate patient information for claim processing, and discrepancies or errors can result in denials. Providers should ensure that they obtain and verify accurate patient information for each claim submission.
To prevent incorrect patient information denials, providers should implement robust patient registration and verification processes that capture accurate patient information. Regular staff training and education on the importance of accurate patient information can help minimize errors. Verification of patient demographics and insurance information at each visit can help ensure that accurate information is collected for claim submission.
Non-Covered Service Denials
Non-covered service denials occur when a service or procedure rendered to a patient is not covered under the patient’s insurance policy. Insurance companies have specific coverage policies that outline what services, procedures, or treatments they consider covered. Providers should verify the patient’s coverage and eligibility for specific services before rendering them.
To prevent non-covered service denials, providers should have a clear understanding of the insurance policies they work with and their coverage criteria. Clear communication with the patient is essential to ensure that they understand what services are covered under their insurance policy and what may be considered non-covered. When there is uncertainty regarding coverage, obtaining a predetermination or prior authorization from the insurance company can help clarify any potential coverage issues.
Reason Denials
Pre-Authorization Denials
Pre-authorization denials occur when a provider submits a claim for services or procedures that require pre-authorization, but the insurance company denies the authorization request. Verification of pre-authorization requirements and obtaining proper pre-authorization from the insurance company before rendering services is crucial to avoid pre-authorization denials. Failure to obtain pre-authorization can leave the provider responsible for the charges.
To prevent pre-authorization denials, providers should familiarize themselves with each insurance company’s specific requirements for pre-authorization. They should also ensure that all necessary documentation, such as medical records or supporting documents, is submitted with the pre-authorization request. Clear communication between the provider and the insurance company is crucial to avoid any misunderstandings or delays in obtaining pre-authorization.
Invalid Diagnosis Denials
Invalid diagnosis denials occur when the diagnosis reported on the claim form is deemed incorrect or invalid by the insurance company. Insurance companies have specific guidelines and criteria for valid diagnoses, and discrepancies or errors can result in denials. Providers should ensure that their coding accurately reflects the patient’s diagnosis and matches the required criteria of the insurance company.
To prevent invalid diagnosis denials, providers should invest in regular training and education for their coding staff to ensure accurate coding practices. The use of comprehensive coding manuals and software that includes coding tips and guidelines can also help minimize errors. Regular audits of coding practices can assist in identifying any potential invalid diagnosis issues and rectify them promptly.
Procedure Not Covered Denials
Procedure not covered denials occur when a procedure or service rendered to a patient is not covered under the patient’s insurance policy. Insurance companies have specific coverage policies that outline what services, procedures, or treatments they consider covered, and discrepancies or errors can result in denials. Providers should verify the patient’s coverage and eligibility for specific procedures before rendering them.
To prevent procedure not covered denials, providers should familiarize themselves with the insurance policies they work with and their coverage criteria. Clear communication with the patient is essential to ensure that they understand what procedures are covered under their insurance policy. When there is uncertainty regarding coverage, obtaining a predetermination or prior authorization from the insurance company can help clarify any potential coverage issues.
Exceeded Benefit Limit Denials
Exceeded benefit limit denials occur when a patient’s insurance coverage has reached its limit or maximum benefit for a specific service or procedure. Insurance policies often have limits on coverage amounts, such as annual maximums or visit limits for certain services. Providers should verify the patient’s coverage and ensure that the services provided are within the allowed limits to avoid exceeded benefit limit denials.
To prevent exceeded benefit limit denials, providers should thoroughly review the patient’s insurance policy and coverage before rendering services. Clear communication with the patient about their coverage and financial responsibilities is essential to manage expectations and minimize exceeded benefit limit denials. In cases where there is uncertainty regarding coverage, obtaining a pre-authorization or predetermination from the insurance company can help clarify any potential coverage issues.
Lack of Medical Necessity Denials
Lack of medical necessity denials occur when there is insufficient documentation or evidence to support the medical necessity of the services provided. Insurance companies rely on accurate and comprehensive medical records to determine the validity and medical necessity of the services provided, and deficiencies in documentation can lead to denials.
To prevent lack of medical necessity denials, providers should implement robust documentation practices that capture all necessary information to support the services provided. Clear and detailed documentation should include the patient’s medical history, examination findings, treatment plans, and the rationale for the services provided. Thorough training and education for medical and billing staff on documentation requirements can help minimize deficiencies in documentation.
Documentation Denials
Incomplete Documentation Denials
Incomplete documentation denials occur when there is insufficient or incomplete documentation to support the services or procedures billed on the claim form. Insurance companies rely on accurate and comprehensive medical records to determine the validity and medical necessity of the services provided. Insufficient documentation can result in denials, leaving the provider responsible for the charges.
To prevent incomplete documentation denials, providers should implement robust documentation practices that capture all necessary information to support the services provided. Clear and detailed documentation should include the patient’s medical history, examination findings, treatment plans, and the rationale for the services provided. Regular training and education for medical and billing staff on documentation requirements can help minimize deficiencies in documentation.
Lack of Medical Necessity Documentation Denials
Lack of medical necessity documentation denials occur when there is insufficient documentation or evidence to support the medical necessity of the services provided. Insurance companies rely on accurate and comprehensive medical records to determine the validity and medical necessity of the services provided, and deficiencies in documentation can lead to denials.
To prevent lack of medical necessity documentation denials, providers should implement robust documentation practices that capture all necessary information to support the services provided. Clear and detailed documentation should include the patient’s medical history, examination findings, treatment plans, and the rationale for the services provided. Thorough training and education for medical and billing staff on documentation requirements can help minimize deficiencies in documentation.
Missing Prior Authorization Denials
Missing prior authorization denials occur when a claim is denied because the insurance company did not receive the necessary prior authorization for the services or procedures rendered. Verification of prior authorization requirements and obtaining proper authorization from the insurance company before rendering services is crucial to avoid missing prior authorization denials. Failure to obtain prior authorization can leave the provider responsible for the charges.
To prevent missing prior authorization denials, providers should familiarize themselves with each insurance company’s specific requirements for prior authorization. They should also ensure that all necessary documentation, such as medical records or supporting documents, is submitted with the prior authorization request. Clear communication between the provider and the insurance company is crucial to avoid any misunderstandings or delays in obtaining prior authorization.
Insufficient Documentation Denials
Insufficient documentation denials occur when there is a lack of adequate supporting documentation to substantiate the services or procedures billed on the claim form. Insurance companies rely on accurate and comprehensive medical records to determine the validity and medical necessity of the services provided, and deficiencies in documentation can lead to denials.
To prevent insufficient documentation denials, providers should implement robust documentation practices that capture all necessary information to support the services provided. Clear and detailed documentation should include the patient’s medical history, examination findings, treatment plans, and the rationale for the services provided. Regular training and education for medical and billing staff on documentation requirements can help minimize deficiencies in documentation.
Unreadable Documentation Denials
Unreadable documentation denials occur when the documentation submitted with the claim is illegible or cannot be easily read or understood by the insurance company. Clear and legible documentation is essential for accurate claims processing and to avoid denials. Providers should ensure that all documentation submitted is easily readable and understandable.
To prevent unreadable documentation denials, providers should establish clear documentation guidelines and standards for the organization. Training and education for medical and billing staff on the importance of legible and clear documentation can help minimize errors. Regular audits of documentation practices can assist in identifying any potential issues with the readability of documentation and rectify them promptly.
Coding Denials
Incorrect CPT Code Denials
Incorrect CPT code denials occur when there are errors or inconsistencies in the current procedural terminology (CPT) codes used on the claim form. Incorrect coding can result from errors in selecting the appropriate code, using outdated codes, or misinterpretation of the documentation. Insurance companies rely on accurate coding to determine reimbursement and discrepancies or errors can result in denials.
To prevent incorrect CPT code denials, providers should invest in regular training and education for their coding staff to ensure accurate coding practices. The use of comprehensive coding manuals and coding software can also help minimize coding errors. Regular audits of coding practices can assist in identifying any potential incorrect CPT code issues and rectify them promptly.
Incorrect ICD-10 Code Denials
Incorrect ICD-10 code denials occur when there are errors or inconsistencies in the International Classification of Diseases, Tenth Revision (ICD-10) codes used on the claim form. Incorrect coding can result from errors in selecting the appropriate code, using outdated codes, or misinterpretation of the documentation. Insurance companies rely on accurate coding to determine reimbursement and discrepancies or errors can result in denials.
To prevent incorrect ICD-10 code denials, providers should invest in regular training and education for their coding staff to ensure accurate coding practices. The use of comprehensive coding manuals and coding software can also help minimize coding errors. Regular audits of coding practices can assist in identifying any potential incorrect ICD-10 code issues and rectify them promptly.
Upcoding Denials
Upcoding denials occur when a provider submits a claim using codes that represent a higher level of service than what was actually provided. This can be an intentional or unintentional error and can result in increased reimbursement. Upcoding is considered fraudulent and can lead to severe consequences, including legal and financial penalties. Providers must ensure that their coding accurately reflects the services provided.
To prevent upcoding denials, providers should invest in regular training and education for their coding staff to ensure accurate coding practices. The use of comprehensive coding manuals and coding software can also help minimize upcoding errors. Regular audits of coding practices can assist in identifying any potential upcoding issues and rectify them promptly.
Unbundling Denials
Unbundling denials occur when a provider bills for separate services or procedures that should be billed together under a single code. Insurance companies have specific guidelines for bundling services, and failing to adhere to these guidelines can result in denials. Providers must ensure that their billing practices reflect accurate bundling of services.
To prevent unbundling denials, providers should familiarize themselves with the bundling rules and guidelines of the insurance companies they work with. It is essential to accurately code and bill for services based on the bundling rules, ensuring that services that should be bundled are not billed and charged separately. Regular reviews of billing practices and audits can help identify any potential unbundling issues and rectify them promptly.
Modifier Errors Denials
Modifier errors denials occur when there are errors or inconsistencies in the modifiers used on the claim form. Modifiers provide additional information about the services provided and can affect reimbursement. Incorrect or missing modifiers can result in denials or reduced reimbursement. Providers must ensure that modifiers are used accurately and appropriately.
To prevent modifier errors denials, providers should invest in regular training and education for their coding staff to ensure accurate use of modifiers. The use of comprehensive coding manuals and coding software can also help minimize modifier errors. Regular audits of coding practices can assist in identifying any potential modifier issues and rectify them promptly.
Reimbursement Denials
Fee Schedule Denials
Fee schedule denials occur when a provider’s billed amount exceeds the maximum allowable amount set by the insurance company’s fee schedule. Insurance companies negotiate fee schedules with providers, determining the maximum reimbursement amount for each service or procedure. Providers should be aware of the fee schedule rates for each insurance company to manage their revenue expectations accurately.
To mitigate fee schedule denials, providers can consider negotiating favorable contracts with insurance companies or participating in preferred provider networks. They can also implement sound financial policies that include clear communication to patients about their financial responsibilities, such as co-pays or deductibles. Understanding the fee schedules and reimbursement rates of each insurance company is crucial for accurate billing and reimbursement.
Out of Network Denials
Out of network denials occur when a provider does not have a contractual agreement with an insurance company, resulting in reduced reimbursement or denial of the claim altogether. Providers who are out of network for a particular insurance company may face challenges in obtaining full reimbursement and may need to negotiate separate agreements or contracts to ensure fair reimbursement.
To address out of network denials, providers can consider negotiating contracts with insurance companies to be included in their network. This can help ensure fair reimbursement for services provided. Effective communication with patients about their insurance coverage and financial responsibilities is crucial to manage expectations and minimize out of network denials.
Maximum Benefit Reached Denials
Maximum benefit reached denials occur when a patient’s insurance coverage has reached its maximum benefit or limit for a specific service or procedure. Insurance policies often have limits on coverage amounts, such as annual maximums or visit limits for certain services. Providers should verify the patient’s coverage and ensure that the services provided are within the allowed limits to avoid maximum benefit reached denials.
To prevent maximum benefit reached denials, providers should thoroughly review the patient’s insurance policy and coverage before rendering services. Clear communication with the patient about their coverage and financial responsibilities is essential to manage expectations and minimize maximum benefit reached denials. In cases where there is uncertainty regarding coverage, obtaining a pre-authorization or predetermination from the insurance company can help clarify any potential coverage issues.
Managed Care Denials
Managed care denials occur when a provider submits a claim to a managed care organization (MCO) that does not have a contract or agreement with the provider. Managed care organizations typically require providers to have a contract and participate in their network to ensure proper reimbursement. Providers should verify their participation status with the MCO and establish contractual agreements if necessary.
To prevent managed care denials, providers should verify their participation status with each managed care organization they work with. Clear communication with the patient about their insurance coverage and financial responsibilities is essential to manage expectations and minimize managed care denials. Negotiating contracts or agreements with managed care organizations can ensure proper reimbursement and reduced denials.
Billing Errors Denials
Billing errors denials occur when there are errors or inconsistencies in the billing processes, such as inaccurate coding, incorrect patient information, or lack of proper documentation. These errors can result in denials or delays in reimbursement. Providers should establish robust billing processes that prioritize accuracy and adherence to billing guidelines.
To prevent billing errors denials, providers should invest in regular training and education for their billing staff to ensure accurate billing practices. The use of comprehensive billing software or systems that can validate claims before submission can help identify and correct errors. Regular audits of billing processes can assist in identifying any potential billing errors and rectify them promptly.
In conclusion, there are various types of denials in medical billing, each with its unique reasons and challenges. Providers must understand the different denial types, establish robust processes and protocols, and invest in staff training and education to reduce denials and improve revenue cycle management. By addressing each denial type and implementing proactive strategies, providers can strive for optimal reimbursement and minimize financial losses.
A clinical coder plays a crucial role in the healthcare industry by analyzing medical records and assigning detailed numerical codes to each diagnosis, treatment, and procedure performed on a patient. These codes serve as a standardized language that allows healthcare providers, researchers, and insurance companies to track, analyze, and make informed decisions based on patient data. With meticulous attention to detail and an in-depth understanding of medical terminology and coding guidelines, a clinical coder ensures accuracy and completeness in the documentation of patient encounters. The proficiency of a clinical coder greatly impacts the quality of healthcare provided, reimbursement rates, and the overall efficiency of healthcare systems.
What Is a Clinical Coder
This image is property of www.rasmussen.edu.
Definition of a Clinical Coder
A clinical coder is a healthcare professional responsible for translating medical diagnoses, procedures, and treatment details into a standardized system of codes. These codes are used for various purposes, such as medical billing, healthcare management, clinical research, and public health analysis. Clinical coders play a crucial role in ensuring accurate and consistent documentation of patient encounters and are highly valued members of the healthcare team.
Role and Responsibilities
The primary role of a clinical coder is to review healthcare documentation, such as physician notes, test results, and other medical records, and assign the appropriate codes according to coding classification systems. This task requires in-depth knowledge of medical terminology, disease processes, and procedures. Clinical coders also ensure the accuracy and completeness of the coded information, as it directly impacts medical billing, reimbursement, and data analysis.
In addition to coding, clinical coders may be involved in data quality assurance, conducting audits to verify the accuracy of coded information, and identifying any inconsistencies or errors. They may collaborate with healthcare providers, administrators, and insurance companies to clarify documentation and ensure compliance with coding guidelines and regulations. Clinical coders must also stay updated with changes in coding systems, guidelines, and regulations to maintain accuracy and efficiency in their work.
Importance of Clinical Coding
Clinical coding is an essential component of modern healthcare systems due to its pivotal role in various aspects of healthcare delivery and management. Accurate coding facilitates seamless communication between healthcare providers, payers, and researchers, ensuring appropriate billing, reimbursement, and analysis of medical data. Here are some key reasons why clinical coding is vital in the healthcare industry:
Medical Billing and Reimbursement: Clinical coding forms the basis for medical billing and reimbursement processes. Accurate coding enables healthcare facilities to receive proper payment for services rendered to patients while ensuring compliance with billing regulations and guidelines.
Clinical Research: Clinical coders provide the data infrastructure necessary for meaningful clinical research. Coded information allows researchers to analyze patient populations, disease patterns, treatment effectiveness, and outcomes, leading to advancements in medical knowledge and improved patient care.
Healthcare Management: Coded data plays a crucial role in healthcare management by providing insights into healthcare utilization, resource allocation, and quality assessment. By analyzing coded data, healthcare administrators can make informed decisions regarding staffing, equipment, and improvements in patient care processes.
Public Health and Epidemiology: Clinical coding is vital in public health analysis and epidemiological studies. Coded data can help identify disease trends, monitor public health emergencies, and contribute to disease surveillance efforts. This information is invaluable in developing effective public health policies and interventions.
Given the importance of clinical coding, it is essential to understand the education, training, and skills required to excel in this field.
Education and Training
Qualifications Required
To become a clinical coder, a minimum educational requirement is a high school diploma or equivalent. However, many employers prefer candidates with additional qualifications, such as an associate’s or bachelor’s degree in health information management or a related field. These educational programs provide students with a solid foundation in medical terminology, anatomy, physiology, and healthcare information systems.
Specialized Training
While formal education provides a fundamental understanding of healthcare and coding principles, specialized training in clinical coding is necessary to develop the skills and knowledge required for accurate code assignment. Many organizations offer coding training programs that focus on coding classification systems, such as the International Classification of Diseases (ICD), Current Procedural Terminology (CPT), and the Healthcare Common Procedure Coding System (HCPCS).
Clinical coders may also receive on-the-job training to familiarize themselves with the specific coding guidelines and software used in their healthcare facility. This training includes hands-on practice, feedback, and mentorship from experienced coders to enhance coding proficiency and accuracy.
Professional Certifications
Obtaining professional certifications in clinical coding is highly recommended to demonstrate expertise and enhance career prospects. Certifications, such as the Certified Coding Specialist (CCS) or Certified Professional Coder (CPC), are offered by reputable organizations and require passing a comprehensive exam. These certifications validate the coder’s knowledge and competence in coding systems, guidelines, and ethical considerations.
Certified clinical coders often have a competitive edge in the job market and may be eligible for higher-paying positions or opportunities for advancement in their careers.
Skills and Competencies
Successful clinical coders possess a unique set of skills and competencies that enable them to perform their roles effectively. Here are some essential skills required for clinical coding:
Medical Knowledge
A strong foundation in medical terminology, anatomy, physiology, and disease processes is essential for accurate code assignment. Clinical coders must understand the clinical context of patient encounters and be able to interpret healthcare documentation to assign the appropriate codes.
Analytical Skills
Clinical coding involves analyzing complex medical records and determining the most suitable codes based on the documentation provided. Coders must be able to assess multiple pieces of information, identify patterns, and apply coding guidelines to ensure accurate code assignment.
Attention to Detail
Precise and meticulous attention to detail is crucial for clinical coders. They need to examine medical documents thoroughly, identifying the relevant information, and selecting the appropriate codes. Even minor errors or omissions can have significant consequences for billing, reimbursement, and data analysis.
Coding Systems and Software Proficiency
Proficiency in coding classification systems, such as ICD, CPT, and HCPCS, is essential. Clinical coders must have a deep understanding of the guidelines and conventions associated with these code sets. Additionally, they should be familiar with coding software and electronic health record (EHR) systems to efficiently navigate and extract necessary information.
Teamwork and Communication
Clinical coders often collaborate with healthcare providers, administrators, and insurance companies. Effective communication and teamwork skills are essential to clarify documentation, resolve coding queries, and address any discrepancies or inconsistencies. Coders must be able to communicate complex coding concepts in a clear and concise manner to ensure clarity and accuracy.
With the necessary education, training, and skills in place, clinical coders can effectively carry out the clinical coding process.
Clinical Coding Process
The clinical coding process involves several sequential steps from the patient encounter to final code assignment. Each step is crucial to ensure accurate and comprehensive documentation. Here are the key steps involved in the clinical coding process:
Patient Encounter
The clinical coding process begins with the patient encounter. This typically involves a healthcare provider examining the patient, conducting tests or procedures, and documenting relevant medical information. These encounters can occur in various healthcare settings, such as hospitals, clinics, or ambulatory care centers.
Healthcare Documentation
Healthcare documentation includes all the records and documents related to the patient encounter. This can include physician notes, test results, imaging reports, operative reports, and other relevant medical records. Clinical coders must thoroughly review these documents to extract the necessary information for code assignment.
Coding Classification Systems
Clinical coders utilize standardized coding classification systems, such as the International Classification of Diseases (ICD), to assign codes to diagnoses and procedures. The ICD provides a comprehensive framework for classifying diseases, conditions, injuries, and external causes. It helps coders accurately capture the patient’s condition and the services provided.
In addition to ICD, clinical coders also use coding systems like the Current Procedural Terminology (CPT) and the Healthcare Common Procedure Coding System (HCPCS) to assign codes to procedures, treatments, and healthcare supplies.
Code Assignment
Based on the healthcare documentation and coding classification systems, clinical coders determine the appropriate codes for each diagnosis, procedure, or treatment. They follow specific coding guidelines, conventions, and instructions provided by coding manuals to ensure accurate code assignment.
Accuracy and Data Quality Assurance
Once the codes are assigned, clinical coders play a critical role in ensuring the accuracy and quality of the coded data. They conduct audits and quality checks to verify the completeness, consistency, and accuracy of the coded information. This step is crucial to avoid billing errors, improve data integrity, and support meaningful data analysis.
Clinical coding guidelines provide coders with standardized rules and conventions for code assignment.
Clinical Coding Guidelines
To ensure consistency and accuracy in code assignment, clinical coders rely on established guidelines and standards. These guidelines help coders interpret healthcare documentation and apply the appropriate codes. Here are some important clinical coding guidelines used globally:
International Classification of Diseases (ICD)
The ICD is the most widely used system for coding diagnoses in healthcare. It provides a list of codes and descriptions for diseases, conditions, injuries, and external causes. Clinical coders refer to the ICD guidelines to accurately assign the appropriate diagnosis code based on the patient’s medical condition.
Current Procedural Terminology (CPT)
CPT is a coding system developed by the American Medical Association (AMA) and is used to code procedures, treatments, and services performed by healthcare providers. CPT codes are essential for reimbursement and billing purposes. Coders rely on CPT guidelines to assign the appropriate procedural codes based on the services provided.
Healthcare Common Procedure Coding System (HCPCS)
HCPCS is another coding system used for reporting medical procedures, supplies, and services provided to Medicare and Medicaid beneficiaries. It includes a vast range of codes for durable medical equipment, ambulance services, and other healthcare items. Coders use HCPCS codes when billing services to government-sponsored healthcare programs.
Local Coding Guidelines
In addition to global coding guidelines, healthcare facilities may establish their own local coding guidelines. These guidelines address specific coding conventions, documentation requirements, and facility-specific coding practices. Coders must adhere to these guidelines to ensure consistency and compliance within their respective healthcare organization.
Understanding and following these coding guidelines is essential for accurate and consistent clinical coding.
Importance in Healthcare
Clinical coding has a significant impact on various aspects of healthcare delivery, management, and research. Let’s explore some key areas where clinical coding plays a vital role:
Medical Billing and Reimbursement
Accurate clinical coding is crucial for medical billing and reimbursement processes. Healthcare facilities rely on coded data to generate accurate invoices and submit claims to insurance companies or government payers. Incorrect or incomplete coding can lead to claim denials, delayed payments, or underbilling, affecting the financial viability of healthcare organizations.
By ensuring accurate coding, clinical coders facilitate proper reimbursement and support the financial sustainability of healthcare facilities.
Clinical Research
Clinical coding provides the foundation for meaningful research and analysis of healthcare data. Researchers rely on coded data to identify patient populations, analyze disease trends, evaluate treatment outcomes, and develop evidence-based guidelines. Robust clinical coding enables researchers to conduct epidemiological studies, clinical trials, and population health analysis.
By translating complex medical information into standardized codes, clinical coders contribute to advancements in medical knowledge, improved patient care, and the development of innovative treatments.
Healthcare Management
Clinical coding plays a crucial role in healthcare management and resource allocation. Coded data provides valuable insights into healthcare utilization, service demand, and patient outcomes. Healthcare administrators and policymakers use this information to make informed decisions regarding staffing levels, resource allocation, and improvements in patient care processes.
Accurate and comprehensive coding data allows healthcare facilities to optimize workflows, improve patient outcomes, and enhance the overall quality of care.
Public Health and Epidemiology
Clinical coding is vital in public health analysis and the tracking of disease patterns. Coded data helps public health officials monitor trends, identify outbreaks, and plan appropriate interventions. By analyzing data across populations, clinical coders contribute to disease surveillance efforts, support public health policies, and enable more effective responses to public health emergencies.
The accurate and consistent coding ensures that public health agencies receive reliable and timely information to protect and improve the health of communities.
Given the significant role of clinical coding and its implications in various healthcare domains, there are numerous career opportunities available for skilled clinical coders.
Career Opportunities
Clinical coders can pursue a diverse range of career opportunities in different healthcare settings and roles. Some of the common career paths for clinical coders include:
Healthcare Facilities
Clinical coders are employed in various healthcare facilities, such as hospitals, clinics, ambulatory care centers, and long-term care facilities. They collaborate closely with physicians, nurses, and other healthcare professionals to ensure accurate and timely coding and documentation.
In these settings, clinical coders may focus on a specific specialty, such as inpatient coding, outpatient coding, or coding for a particular department, such as cardiology or oncology. Career progression opportunities may include supervisory roles, coding management, or involvement in coding audits and compliance.
Health Information Management
Health information management (HIM) departments within healthcare facilities often employ clinical coders. In this role, clinical coders may be responsible for coding, medical record review, coding quality assurance, or data analysis. HIM professionals ensure the accuracy, integrity, and security of healthcare data, including clinical coding data.
Health information management offers various career paths, including HIM director, coding manager, clinical documentation improvement specialist, or coding compliance officer. These roles often involve leadership, strategic planning, and staff education to maintain coding accuracy and compliance.
Insurance Companies
Insurance companies hire clinical coders to evaluate claims for medical services and ensure proper coding and billing practices. Coders working in insurance companies review healthcare documentation provided by healthcare providers and verify the accuracy and appropriateness of the coded information.
Working in insurance coding allows clinical coders to gain insight into the reimbursement processes, billing regulations, and insurance industry standards. They may also have opportunities to contribute to coding policy development, coding audits, and training programs.
Consulting Firms
Clinical coders with expertise in coding systems, regulations, and documentation may find opportunities in healthcare consulting firms. These firms provide a range of services to healthcare organizations, including coding audits, compliance reviews, revenue cycle management, and process improvement.
Working in consulting allows clinical coders to work with multiple clients, gain exposure to diverse healthcare settings, and contribute to improving coding practices, compliance, and financial performance of healthcare organizations.
Future Trends in Clinical Coding
As technology continues to advance and healthcare systems evolve, the field of clinical coding is also undergoing significant changes. Here are some emerging trends that will shape the future of clinical coding:
Automated Coding Systems
Advancements in natural language processing, machine learning, and artificial intelligence have paved the way for automated coding systems. These systems use algorithms to analyze healthcare documentation and propose codes based on the content. While human validation and oversight will still be necessary, automated coding systems have the potential to streamline coding processes, improve accuracy, and reduce coding backlogs.
Artificial Intelligence in Coding
Beyond automated coding systems, artificial intelligence (AI) holds promise in enhancing clinical coding accuracy and efficiency. AI models can learn from vast amounts of coded data, identify coding patterns, and suggest appropriate codes for complex scenarios. With AI assistance, clinical coders can expedite their workflow, focus on more complex coding issues, and ensure standardized code assignment.
Electronic Health Records (EHR)
EHR systems have become ubiquitous in healthcare settings, providing a comprehensive platform for healthcare documentation and information exchange. Integration of coding tools within EHR systems enables real-time coding, automated code suggestion, and immediate feedback on coding accuracy. Future developments in EHR systems will further enhance clinical coding capabilities and improve workflow efficiency.
Data Analytics and Reporting
Clinical coders’ expertise in coding and medical data interpretation uniquely positions them to contribute to data analytics and reporting. Coders can leverage their understanding of coding systems and disease classifications to granularly analyze healthcare data, identify trends, and generate insightful reports. The ability to transform coded data into meaningful information will continue to be in high demand as healthcare moves towards evidence-based decision-making and population health management.
While the future of clinical coding holds exciting possibilities, it also presents challenges and ethical considerations that coders must navigate.
Challenges and Ethical Considerations
Clinical coding comes with its fair share of challenges and ethical dilemmas. Here are some key considerations faced by clinical coders:
Coding Accuracy and Consistency
Maintaining consistent coding accuracy is a continuous challenge for clinical coders. Classification systems, guidelines, and regulations undergo frequent updates, requiring coders to stay updated with changes. Accurately interpreting physician documentation, especially in complex cases, can also be challenging, as different providers may use varying terminology or coding conventions.
Coders must continuously invest in their professional development, seek clarification when necessary, and participate in coding quality assurance initiatives to mitigate coding errors and ensure consistent and accurate code assignment.
Confidentiality and Privacy
Clinical coders have access to sensitive patient information and must adhere to strict confidentiality and privacy regulations. They are bound by ethical and legal obligations to protect patient privacy when handling medical records. Coders must prioritize patient confidentiality throughout the coding process and take necessary precautions to safeguard protected health information.
Ethical Dilemmas
Clinical coding may present ethical dilemmas, such as ambiguous documentation, conflicting coding guidelines, or coding for uncertain diagnoses. Coders must follow established ethical guidelines and seek guidance from supervisors, coding committees, or professional organizations when faced with such dilemmas. Open communication and ethical decision-making are essential to ensure accurate and ethical coding practices.
Continuous Learning and Keeping Updated
The field of clinical coding is ever-evolving, with regular updates to coding systems, guidelines, and regulations. Clinical coders must demonstrate a commitment to lifelong learning, staying updated with changes, and engaging in professional development activities. This includes attending coding conferences, participating in coding webinars, and maintaining memberships with professional organizations to ensure continuous growth and competence.
Conclusion
Clinical coding is a vital function in healthcare, ensuring accurate representation and communication of patient encounters through standardized codes. Clinical coders play a crucial role in medical billing, clinical research, healthcare management, and public health analysis. The importance of this role cannot be overstated, as it impacts various aspects of healthcare delivery and decision-making.
Clinical coders require a combination of medical knowledge, analytical skills, attention to detail, coding system proficiency, and effective communication. They follow a comprehensive coding process, adhere to coding guidelines, and contribute to data accuracy and quality assurance. Clinical coding career opportunities exist in healthcare facilities, health information management, insurance companies, and consulting firms, providing a diverse range of roles and responsibilities.
The future of clinical coding holds exciting possibilities, such as automated coding systems, artificial intelligence integration, and advanced data analytics. However, coders must also navigate challenges relating to accuracy, confidentiality, ethical dilemmas, and continuous learning.
In conclusion, the role of a clinical coder is crucial in ensuring accurate documentation, proper reimbursement, and valuable medical data for research and public health. The dedicated efforts of clinical coders contribute to better patient care, improved healthcare management, and advancements in medical science.
This image is property of www.northwestcareercollege.edu.
In the field of medical coding, it is important to understand the concept of eponym medical coding, which refers to coding procedures or diagnoses based on the name of a person who discovered a particular disease, surgical technique, or medical condition. An example of an eponym medical coding is “Parkinson’s disease,” named after the British physician James Parkinson who first described the symptoms and characteristic features of this neurodegenerative disorder. By understanding eponym medical coding, healthcare professionals can accurately identify and classify various medical conditions and procedures, ensuring effective communication and efficient healthcare delivery.
Definition of Eponym Medical Coding
Eponym medical coding refers to the practice of labeling diseases, medical conditions, and procedures with the name of the person who first described or discovered them. These names are coined after individuals who play a significant role in the advancement of medical knowledge and research. Eponym medical coding provides a standardized way to identify and classify various medical conditions, allowing for improved communication and understanding among healthcare professionals.
This image is property of www.educationworld.in.
Understanding Eponym Medical Coding
Eponym medical coding involves using the name of an individual as a reference point to identify certain diseases or medical conditions. This coding system acknowledges the contributions made by these individuals to the field of medicine. By using eponyms, medical professionals can easily recognize and discuss specific conditions, which helps in making accurate diagnoses, providing appropriate treatment plans, and conducting effective research.
This image is property of www.mrahis.com.
Importance of Eponym Medical Coding
Eponym medical coding holds significant importance in the medical field for several reasons. First, it provides a time-honored tradition of recognizing and honoring the individuals who have made invaluable contributions to medical science. By associating their names with specific diseases or conditions, their legacies are preserved and celebrated.
Second, eponym coding enhances communication among healthcare professionals. When discussing a particular condition using eponyms, medical professionals can quickly understand and convey important information. This facilitates efficient collaboration and ensures accurate transmission of medical knowledge.
Third, eponym coding serves as a mnemonic aid, aiding in the retention and recall of medical information. By associating a condition with an individual’s name, healthcare professionals are more likely to remember and recognize specific medical conditions, which ultimately facilitates accurate diagnoses and treatment decisions.
Moreover, eponym coding promotes the identification and awareness of rare diseases or conditions. By using eponyms, these lesser-known conditions become more easily recognizable, leading to prompt diagnosis and appropriate treatment. This can significantly impact patient outcomes and the availability of targeted resources and support.
Example of Eponym Medical Coding
Numerous medical conditions are labeled with eponyms to honor the individuals who played a crucial role in their identification and characterization. Let’s explore some prominent examples below:
Parkinson’s Disease (PD)
Parkinson’s disease, a neurodegenerative disorder that affects movement and coordination, is named after James Parkinson. In 1817, Parkinson published a pioneering work, “An Essay on the Shaking Palsy,” which outlined the clinical features and progression of the disease.
Lou Gehrig’s Disease (ALS)
Amyotrophic Lateral Sclerosis (ALS), also known as Lou Gehrig’s disease, is named after the famous baseball player who was diagnosed with the condition in 1939. Gehrig’s courage and advocacy raised awareness about this progressive neurodegenerative disease, which affects the nerve cells responsible for controlling voluntary muscle movement.
Down Syndrome
Down syndrome, a genetic disorder causing developmental and intellectual delays, is named after the British physician John Langdon Down. Dr. Down observed and described the characteristic features of the condition in 1866, contributing significantly to our understanding of this congenital disorder.
Hodgkin’s Lymphoma
Hodgkin’s lymphoma, a type of cancer affecting the lymphatic system, is named after the physician Thomas Hodgkin. In the early 19th century, Hodgkin conducted extensive research on lymphomas and identified distinct characteristics of this particular cancer, leading to its recognition as a distinct clinical entity.
Crohn’s Disease
Crohn’s disease, an inflammatory bowel disease, is named after Dr. Burrill B. Crohn. Along with his colleagues, Crohn extensively researched and described the features of the disease in 1932, shedding light on its clinical presentation, pathology, and treatment options.
Asperger’s Syndrome
Asperger’s syndrome, a developmental disorder characterized by difficulties in social interactions and repetitive patterns of behavior, is named in honor of Hans Asperger. Asperger’s early work in the 1940s significantly contributed to the field of autism research, leading to the recognition of this distinct condition.
Alzheimer’s Disease
Alzheimer’s disease, a progressive neurological disorder causing cognitive decline and memory loss, is named after the German psychiatrist Alois Alzheimer. Alzheimer’s observations and detailed case studies published in 1906 significantly advanced our understanding of this debilitating disease.
Peyronie’s Disease
Peyronie’s disease, a condition characterized by the abnormal curvature of the penis during erections, is named after the French physician François Gigot de la Peyronie. In the 18th century, Peyronie documented several cases and described the condition, making significant contributions to its understanding.
Kaposi’s Sarcoma
Kaposi’s sarcoma, a rare cancer affecting the blood vessels, is named after the Hungarian dermatologist Moritz Kaposi. In the late 19th century, Kaposi provided detailed descriptions of the disease, which primarily affects individuals with weakened immune systems or specific viral infections.
Apgar Score
The Apgar score, a quick assessment of a newborn’s overall condition, is named after the American anesthesiologist Virginia Apgar. Apgar developed the scoring system in 1952 to evaluate a newborn’s vital signs, including heart rate, breathing, muscle tone, reflexes, and skin color, immediately after birth.
In conclusion, eponym medical coding is an essential aspect of medical terminology, honoring the individuals who have made significant contributions to the field. By using eponyms, healthcare professionals can better communicate, remember, and diagnose specific medical conditions. Furthermore, eponym coding highlights rare diseases, elevating their visibility and enabling timely interventions. The examples mentioned above demonstrate the pervasive influence of eponym medical coding across a wide range of medical conditions, allowing for a more comprehensive understanding of the medical landscape.
In the world of medical billing, understanding the various types of modifiers is crucial for accurate and efficient processing of claims. Modifiers play a significant role in defining the specific circumstances and conditions of a medical procedure or service. By appending the appropriate modifier to a claim, healthcare providers can ensure rightful reimbursement and avoid potential denials or inaccuracies. This article will explore the different types of modifiers commonly used in medical billing, shedding light on their purpose and significance in the intricate world of healthcare reimbursement.
Modifiers in Medical Billing
Modifiers play a crucial role in medical billing, allowing healthcare providers to accurately communicate the specific circumstances of a procedure or service to insurance payers. These modifiers consist of a two-digit code appended to a CPT (Current Procedural Terminology) code, providing additional information about the nature of the procedure or service performed. Understanding the various types of modifiers is essential for healthcare professionals involved in medical billing, ensuring proper reimbursement and avoiding potential claim denials. In this article, we will explore the different types of modifiers used in medical billing, their importance, and their specific purposes in various healthcare settings.
Evaluation and Management Modifiers
Evaluation and Management (E&M) services are essential components of medical practice, involving the assessment, diagnosis, and management of patients. Modifiers associated with E&M services serve to highlight unique circumstances or significant aspects of these encounters. Three commonly used E&M modifiers include Modifier 25, Modifier 57, and Modifier 59.
Modifier 25: Significant, Separately Identifiable Evaluation and Management Service by the Same Physician on the Same Day of the Procedure Modifier 25 is used when a significant E&M service is provided by the same physician on the same day as a procedure. This modifier ensures that the E&M service is recognized and reimbursed separately from the procedure.
Modifier 57: Decision for Surgery Modifier 57 indicates that the E&M service resulted in the decision to perform surgery, highlighting the vital role of the physician’s evaluation and decision-making process. This modifier helps prevent bundling of the E&M service with the subsequent surgical procedure.
Modifier 59: Distinct Procedural Service Modifier 59 is commonly used to identify procedures or services that are distinct and separate from each other, preventing them from being bundled into a single reimbursement. This modifier is particularly useful for situations where multiple procedures are performed during the same encounter, but each procedure has a distinct purpose or anatomical location.
This image is property of www.veralon.com.
Surgical Modifiers
surgical modifiers are essential in medical billing to accurately describe various aspects of surgical procedures. These modifiers provide important details, such as increased complexity, postoperative management, and unexpected returns to the operating room. Common surgical modifiers include Modifier 22, Modifier 24, and Modifier 78.
Modifier 22: Increased Procedural Service Modifier 22 is used when a procedure requires additional work beyond the typical circumstances outlined in the CPT code description. This modifier is appropriate when a procedure entails increased complexity, increased intensity, or additional time and effort on the part of the physician.
Modifier 24: Unrelated Evaluation and Management Service by the Same Physician During a Postoperative Period Modifier 24 is used to indicate that an unrelated evaluation and management service was provided by the same physician during a postoperative period. This modifier ensures that the physician is appropriately reimbursed for any additional services rendered during this period that are not directly related to the surgical procedure.
Modifier 78: Unplanned Return to the Operating/Procedure Room by the Same Physician or Other Qualified Healthcare Professional Following Initial Procedure for a Related Procedure Modifier 78 is used to signify an unplanned return to the operating/procedure room by the same physician or other qualified healthcare professional for a related procedure. This modifier ensures that the subsequent procedure is recognized and reimbursed separately from the initial procedure.
Anesthesia Modifiers
Anesthesia services require specific modifiers to accurately document the involvement of the surgeon and any unexpected circumstances that may arise during the procedure. Two important anesthesia modifiers are Modifier 47 and Modifier 53, along with the previously discussed Modifier 78 in the surgical section.
Modifier 53: Discontinued Procedure Modifier 53 is used when a procedure is started but discontinued due to extenuating circumstances or patient factors that prevent its completion. This modifier allows for appropriate reimbursement for the portion of the procedure performed.
Modifier 78: Return to the Operating/Procedure Room for a Related Procedure During the Postoperative Period As mentioned earlier in the surgical section, Modifier 78 is used when there is an unplanned return to the operating/procedure room for a related procedure during the postoperative period.
Radiology Modifiers
Modifiers in radiology billing help differentiate between the professional and technical components of a radiology service or identify distinct procedural services. The two primary radiology modifiers are Modifier 26 and Modifier TC, along with the previously discussed Modifier 59 used for distinct procedural services.
Modifier 26: Professional Component Modifier 26 is used to indicate that the healthcare professional provided only the professional component of a radiology service, such as interpreting and providing a written report. This modifier ensures appropriate reimbursement for the professional component alone.
Modifier TC: Technical Component Modifier TC indicates that the healthcare professional provided only the technical component of a radiology service, such as the equipment, facilities, and technician that performed the imaging. This modifier ensures appropriate reimbursement for the technical component alone.
Pathology and Laboratory Modifiers
Pathology and laboratory services require specific modifiers to indicate certain circumstances, such as reference to outside laboratories, repeat tests, and the use of multiple modifiers. Commonly used pathology and laboratory modifiers include Modifier 90, Modifier 91, and Modifier 99.
Modifier 90: Reference (Outside) Laboratory Modifier 90 is used when laboratory testing is performed by an outside laboratory, rather than in-house. This modifier ensures appropriate reimbursement for the use of external laboratory services.
Modifier 91: Repeat Clinical Diagnostic Laboratory Test Modifier 91 is used when a laboratory test is repeated on the same patient, same day, and same encounter. This modifier assists in accurate reimbursement for repetitive tests that provide essential diagnostic information.
Modifier 99: Multiple Modifiers Modifier 99 is used when multiple modifiers are necessary to fully describe a procedure or service. This modifier helps eliminate any confusion or potential coding errors due to the use of multiple modifiers.
This image is property of upload.orthobullets.com.
Medicine Modifiers
Medicine modifiers are essential for accurately coding and billing for a wide range of medical services and procedures. These modifiers are used to indicate multiple outpatient encounters, distinct procedural services, and repeat procedures. Notable medicine modifiers include Modifier 27, Modifier 59, and Modifier 76.
Modifier 27: Multiple Outpatient Hospital E/M Encounters on the Same Date Modifier 27 is used when multiple Evaluation and Management encounters occur in an outpatient hospital setting on the same date. This modifier ensures appropriate reimbursement for each separate E&M encounter.
Modifier 59: Distinct Procedural Service As previously discussed in the evaluation and management and radiology sections, Modifier 59 is also used in medicine billing to identify distinct procedural services. It prevents inappropriate bundling of procedures that are separate and independently reportable.
Modifier 76: Repeat Procedure or Service by Same Physician or Other Qualified Healthcare Professional Modifier 76 is used when the same physician or other qualified healthcare professional performs a repeat procedure or service. This modifier ensures proper reimbursement for subsequent procedures or services necessary for the patient’s care.
Physical Therapy Modifiers
Physical therapy services require specific modifiers to accurately depict the delivery of outpatient physical therapy, occupational therapy, and speech-language pathology care. These modifiers differentiate between the various types of therapy plans. Key physical therapy modifiers include Modifier GP, Modifier GO, and Modifier GN.
Modifier GP: Services Delivered Under an Outpatient Physical Therapy Plan of Care Modifier GP is used to indicate that services were delivered under an outpatient physical therapy plan of care. This modifier ensures accurate billing for physical therapy services performed and helps differentiate them from other types of therapy services.
Modifier GO: Services Delivered Under an Outpatient Occupational Therapy Plan of Care Modifier GO is used when services are delivered under an outpatient occupational therapy plan of care. This modifier facilitates proper reimbursement for occupational therapy services provided and distinguishes them from other therapy services.
Modifier GN: Services Delivered Under an outpatient speech-language pathology plan of care Modifier GN is used to indicate that services were delivered under an outpatient speech-language pathology plan of care. This modifier ensures accurate billing for speech-language pathology services performed and differentiates them from other therapy services.
Ambulance Modifiers
Ambulance services also require specific modifiers to properly describe the type of item or service provided and the expectation of payment denial. The two key ambulance modifiers are Modifier GY and Modifier GZ.
Modifier GY: Item or Service Statutorily Excluded, Does Not Meet the Definition of Any Medicare Benefit or for Non-Medicare Insurers, is Not a Contractual Benefit Modifier GY is used to indicate that the item or service provided is statutorily excluded and does not meet the definition of any Medicare benefit. For non-Medicare insurers, it signifies that the item or service is not a contractual benefit.
Modifier GZ: Item or Service Expected to be Denied as Not Reasonable and Necessary Modifier GZ is used to signify that the item or service provided is expected to be denied as not reasonable and necessary. This modifier alerts insurance payers that the reimbursement for the item or service may be denied based on medical necessity criteria.
Modifiers for Non-Physician Practitioners
Non-physician practitioners, such as nurse practitioners, certified registered nurse anesthetists, and registered dietitians, also use specific modifiers to accurately bill for their services. Noteworthy modifiers for non-physician practitioners include Modifier SA, Modifier SE, and Modifier SG.
Modifier SA: Nurse Practitioner (NP) Services Modifier SA is used to identify services provided by a nurse practitioner (NP). This modifier ensures accurate reimbursement for the services rendered by the NP, distinguishing them from services provided by physicians.
Modifier SE: Certified Registered Nurse Anesthetist (CRNA) Services Modifier SE is used to indicate services provided by a certified registered nurse anesthetist (CRNA). This modifier helps establish appropriate reimbursement for the anesthesia services provided by the CRNA, distinguishing them from those provided by physicians or anesthesiologists.
Modifier SG: Registered Dietitian (RD) Services Modifier SG is used to identify services provided by a registered dietitian (RD). This modifier ensures accurate billing for the services delivered by the RD, differentiating them from services provided by other healthcare professionals.
In conclusion, understanding the different types of modifiers in medical billing is essential for healthcare professionals involved in coding and billing processes. Each modifier serves a unique purpose, accurately communicating specific circumstances, services, or situations that may impact reimbursement. Familiarizing oneself with the appropriate use of modifiers helps ensure compliance, prevent claim denials, and facilitate proper reimbursement in the complex landscape of medical billing.
Medical coding is a fundamental process in the healthcare industry that involves the translation of medical diagnoses, procedures, and treatments into universally recognized codes. These codes serve as a unique language that helps healthcare professionals accurately document and communicate vital patient information. For example, when a patient visits a healthcare provider for a check-up, the physician will assign specific codes to document the visit, diagnostic tests performed, and any procedures or medications prescribed. These codes are crucial for accurate billing purposes, tracking patient outcomes, and conducting clinical research. In essence, medical coding plays a vital role in maintaining effective healthcare delivery and streamlining administrative processes.
This image is property of res.cloudinary.com.
Heading 1
Subheading 1.1
Medical Coding: An Essential Component of the Healthcare Industry
In the world of healthcare, medical coding plays a vital role in ensuring accurate and efficient communication between healthcare providers, insurance companies, and government agencies. Medical coding involves the transformation of medical diagnoses, procedures, and services into universally recognized alphanumeric codes. These codes provide a standardized way of documenting medical information, facilitating proper billing, reimbursement, and data analysis. Without medical coding, the healthcare industry would face significant challenges in managing patient records, conducting research, and ensuring appropriate financial transactions.
Subheading 1.2
Understanding the Purpose and Process of Medical Coding
Medical coding serves various purposes within the healthcare system. Firstly, it allows healthcare providers to record and communicate specific details about a patient’s medical condition and the services provided during a visit or treatment. This information is crucial for providing quality care, coordinating treatment plans, and preserving accurate medical histories. Secondly, coding facilitates accurate billing and reimbursement for healthcare services rendered. Insurance companies and government agencies rely on these codes to determine the appropriate amount to reimburse a healthcare provider. Finally, medical coding plays a key role in data analysis, research, and decision-making within the healthcare industry. It enables the identification of trends, patterns, and outcomes, contributing to advancements in medical science and healthcare delivery.
To ensure uniformity and consistency, medical coding follows specific guidelines and protocols. the coding process typically involves reviewing medical records, extracting relevant information, and assigning the appropriate codes based on the patient’s diagnosis, procedures performed, and any additional factors. This requires skilled medical coders who possess a thorough understanding of anatomy, medical terminology, and coding systems, such as the International Classification of Diseases (ICD) and the Current Procedural Terminology (CPT). With these codes in place, medical records become standardized, facilitating seamless communication and understanding among healthcare professionals.
Heading 2
Subheading 2.1
ICD Coding: Documenting Diagnoses
One example of medical coding is the use of the International Classification of Diseases (ICD) codes to document and categorize diagnoses. The ICD is a globally recognized system that provides a comprehensive list of medical conditions and assigns them unique codes. By correctly applying ICD codes, healthcare professionals can accurately represent a patient’s medical condition, which enhances communication and contributes to improved patient care.
When a patient visits a healthcare provider, the healthcare professional will evaluate their symptoms, conduct tests, and ultimately arrive at a diagnosis. This diagnosis is then translated into an ICD code, which describes the condition using precise language that is universally understood. For instance, if a patient is diagnosed with pneumonia, a specific ICD code, such as J18.9, “Pneumonia, unspecified organism,” may be assigned to indicate the condition. This code captures essential information about the diagnosis, enabling accurate record-keeping and effective communication with other healthcare professionals involved in the patient’s care.
Subheading 2.2
CPT Coding: Documenting Medical Procedures
In addition to diagnosing medical conditions, healthcare providers also perform various procedures to treat their patients. To document these procedures adequately, healthcare professionals utilize Current Procedural Terminology (CPT) codes. CPT codes are numeric codes developed and maintained by the American Medical Association (AMA) and are used to communicate specific medical services performed during a patient encounter.
CPT codes cover a wide range of medical procedures, including surgeries, office visits, laboratory tests, and therapeutic interventions. Each code corresponds to a particular procedure or service, ensuring accurate representation of the healthcare provided. For example, if a patient undergoes a knee arthroscopy, the corresponding CPT code, such as 29881, “Arthroscopy, knee, diagnostic, with or without synovial biopsy (separate procedure),” would be assigned to document the procedure accurately. These codes assist in standardized documentation, billing, and reimbursement processes, enabling efficient workflow and proper financial management within healthcare organizations.
Improved Patient Care: Accurate medical coding ensures that relevant clinical information is properly recorded and easily accessible to healthcare professionals. This promotes better communication, care coordination, and treatment decision-making, ultimately leading to improved patient outcomes.
Proper Reimbursement: Insurance companies, government agencies, and other healthcare payers rely on accurate coding to determine reimbursement amounts for healthcare services. Incorrect coding can result in delayed or denied reimbursement, leading to financial strain for healthcare providers and potential challenges for patients in accessing necessary care.
Billing and Revenue Cycle Management: Accurate coding directly impacts the billing and revenue cycle management process in healthcare organizations. Proper coding contributes to timely and accurate claim submissions, reduced billing errors, and improved cash flow for healthcare providers.
Data Analysis and Research: Accurate coding produces reliable and consistent data, which is vital for healthcare research, tracking disease prevalence, analyzing treatment options, and identifying healthcare trends. Researchers and policymakers heavily rely on coded data to make informed decisions and advancements in healthcare.
Compliance with Regulations: The healthcare industry is subject to various regulations and requirements, such as those set by insurance companies, government agencies, and professional organizations. Accurate coding ensures compliance with these regulations, reducing the risk of penalties, audits, and legal consequences for healthcare providers.
Efficient and precise medical coding is crucial to the success of any healthcare organization, benefiting patients, healthcare professionals, payers, and the overall healthcare system as a whole.
Subheading 3.2
Challenges and Future Trends in Medical Coding
While medical coding plays a pivotal role in the healthcare industry, it is not without its challenges. Some of these challenges include:
Complexity and Updates: Medical coding systems, such as ICD and CPT, are intricate and constantly evolving. Keeping up with coding guidelines, updates, and new codes requires continuous education and training for medical coders.
Coding Errors and Inaccuracies: Mistakes in medical coding can result in claim denials, billing discrepancies, and potentially compromise patient care. Precision and attention to detail are vital to avoid coding errors.
Technology Integration: The implementation of electronic health records (EHRs) and computer-assisted coding (CAC) systems has revolutionized medical coding. However, successfully integrating these technologies and harnessing their full potential can be challenging for healthcare organizations.
As the healthcare industry continues to evolve, medical coding will also undergo changes and advancements. Some of the future trends in medical coding include:
Automation and Artificial Intelligence: Automation and artificial intelligence (AI) have the potential to streamline the coding process, reducing the chances of errors and improving coding accuracy and efficiency.
Electronic Health Records (EHRs): EHR systems are becoming increasingly commonplace, leading to improved documentation and coding capabilities. Integrating coding directly into EHRs can enhance workflow and reduce duplicative efforts.
ICD-11: The transition to the latest edition of the ICD coding system, known as ICD-11, is underway. ICD-11 aims to improve coding accuracy, expand coding capabilities, and enable enhanced data analytics and research.
In conclusion, medical coding is a critical component of the healthcare industry, facilitating accurate communication, billing, reimbursement, and data management. Understanding the purpose, process, and examples of medical coding is essential for healthcare professionals, insurers, researchers, and policymakers alike. Accurate medical coding ensures optimal patient care, efficient operations, and the advancement of medical science. As the healthcare industry evolves, so will medical coding, embracing technological advancements and embracing new coding systems to meet the ever-changing needs of the industry.
In the field of medical billing and coding, there are various certifications that professionals can obtain to enhance their knowledge and credibility. These certifications validate the expertise and competence of individuals in accurately translating medical procedures, diagnoses, and services into codes for billing purposes. By acquiring these certifications, medical billing and coding professionals can demonstrate their commitment to quality and accuracy in their work, ensuring optimal reimbursement for healthcare providers and efficient management of patient records. This article explores the different medical billing and coding certifications available, shedding light on their significance and requirements.
Certified Professional Coder (CPC)
Overview
The Certified Professional Coder (CPC) certification is offered by the American Academy of Professional Coders (AAPC). This certification is highly recognized in the field of medical billing and coding and signifies that you have achieved a high level of proficiency in coding medical diagnoses and procedures using the Current Procedural Terminology (CPT) and International Classification of Diseases (ICD) coding systems. The CPC certification is valuable for individuals who wish to work as professional coders in a wide range of healthcare settings.
Requirements
To become a Certified Professional Coder (CPC), you need to meet certain requirements set by the AAPC. These requirements include a high school diploma or equivalent, a strong understanding of medical terminology and anatomy, and a good grasp of coding guidelines and regulations. Additionally, you must also have at least two years of coding experience or complete an AAPC-approved coding program.
Exam
To obtain the CPC certification, you must pass the CPC exam. This exam consists of questions related to medical coding principles, CPT and ICD coding guidelines, and healthcare regulations. The exam is divided into two parts, with the first part focusing on multiple-choice questions and the second part testing your skills in medical coding. It is essential to thoroughly prepare for the exam by studying coding guidelines and practicing coding scenarios.
Job Prospects
Having a CPC certification opens up a wide range of job opportunities in the field of medical billing and coding. Graduates with this certification can find employment in hospitals, clinics, private practices, insurance companies, and government organizations. With the increasing emphasis on accurate coding and proper reimbursement in healthcare, the demand for CPC-certified professionals is expected to grow.
Salary
The salary for CPC-certified professionals can vary based on factors such as experience, location, and job role. On average, CPC-certified coders earn a competitive salary that reflects their expertise and knowledge in medical coding. According to the AAPC’s Salary Survey, the average annual salary for certified professional coders is around $55,000. However, it is important to note that salaries can range from $40,000 to over $70,000, depending on various factors.
Certified Coding Specialist (CCS)
Overview
The Certified Coding Specialist (CCS) certification is offered by the American Health Information Management Association (AHIMA). This certification is designed for individuals who want to specialize in hospital coding and gain a comprehensive understanding of coding systems, medical terminology, and healthcare reimbursement methodologies. CCS-certified professionals play a crucial role in ensuring accurate coding and proper billing practices for inpatient hospital services.
Requirements
To become a Certified Coding Specialist (CCS), you need to fulfill certain requirements established by AHIMA. These requirements include a high school diploma or equivalent, completion of a coding education program, and a good understanding of medical terminology, anatomy, and healthcare regulations. Additionally, you must also have at least two years of coding experience in a hospital setting or complete an AHIMA-approved coding program.
Exam
To obtain the CCS certification, you must pass the CCS exam. This exam assesses your proficiency in coding medical diagnoses and procedures in an inpatient hospital setting. The exam is divided into multiple-choice questions and medical scenario-based questions, which test your coding knowledge and decision-making skills. It is essential to study coding guidelines and practice coding scenarios to prepare effectively for the exam.
Job Prospects
Being a CCS-certified professional opens up various job opportunities in hospital coding and healthcare information management. CCS-certified individuals can work in hospitals, healthcare consulting firms, government agencies, and other healthcare organizations. The demand for CCS-certified professionals is expected to grow as the healthcare industry continues to rely on accurate coding and billing practices for optimal financial reimbursement.
Salary
The salary for CCS-certified professionals can vary based on factors such as experience, location, and job role. On average, CCS-certified coders earn a competitive salary that reflects their specialized skills in inpatient coding. According to the AHIMA’s salary survey, the average annual salary for CCS-certified professionals is around $70,000. However, salaries can range from $50,000 to over $90,000, depending on various factors.
Certified Professional Biller (CPB)
Overview
The Certified Professional Biller (CPB) certification is offered by the American Academy of Professional Coders (AAPC). This certification is specifically designed for individuals who want to specialize in medical billing. CPB-certified professionals are skilled in various aspects of medical billing, including claim submission, payment processing, reimbursement methodologies, and insurance-related regulations.
Requirements
To become a Certified Professional Biller (CPB), you need to meet certain requirements set by the AAPC. These requirements include a high school diploma or equivalent, a good understanding of medical terminology and billing processes, and knowledge of insurance regulations and coding. Additionally, you must also have at least two years of experience working in medical billing or complete an AAPC-approved billing program.
Exam
To obtain the CPB certification, you must pass the CPB exam. This exam assesses your knowledge and skills in medical billing processes, insurance coverage, reimbursement methodologies, and compliance regulations. The exam consists of multiple-choice questions and covers various topics related to medical billing. It is essential to study billing guidelines and practice billing scenarios to prepare effectively for the exam.
Job Prospects
Having a CPB certification can open up a wide range of job opportunities in medical billing. CPB-certified professionals can work in hospitals, clinics, billing companies, insurance companies, and other healthcare organizations. With the increasing complexity of medical billing practices and insurance regulations, the demand for CPB-certified professionals is expected to grow.
Salary
The salary for CPB-certified professionals can vary based on factors such as experience, location, and job role. On average, CPB-certified billers earn a competitive salary that reflects their expertise in medical billing. According to the AAPC’s Salary Survey, the average annual salary for certified professional billers is around $45,000. However, salaries can range from $35,000 to over $55,000, depending on various factors.
Certified Coding Associate (CCA)
Overview
The Certified Coding Associate (CCA) certification is offered by the American Health Information Management Association (AHIMA). This certification is suitable for entry-level professionals who want to start their career in medical coding. The CCA certification validates the individual’s basic knowledge and skills in accurate medical coding using the ICD coding system.
Requirements
To become a Certified Coding Associate (CCA), you need to fulfill certain requirements established by AHIMA. These requirements include a high school diploma or equivalent and completion of an AHIMA-approved coding education program. It is recommended to have a good understanding of medical terminology and anatomy before pursuing this certification.
Exam
To obtain the CCA certification, you must pass the CCA exam. This exam assesses your knowledge and skills in medical coding and includes multiple-choice questions related to the coding guidelines and healthcare regulations. The CCA certification is a stepping stone for individuals who want to pursue higher-level coding certifications.
Job Prospects
Having a CCA certification can provide you with entry-level job opportunities in medical coding. CCA-certified professionals can work in various healthcare settings, including hospitals, clinics, and outpatient facilities. While the scope of practice for CCA-certified individuals may be more limited compared to higher-level certifications, it serves as a strong foundation for further growth in the field.
Salary
The salary for CCA-certified professionals can vary based on factors such as experience, location, and job role. On average, CCA-certified coders earn a competitive starting salary that reflects their entry-level skills in medical coding. According to the AHIMA’s salary survey, the average annual salary for CCA-certified professionals is around $42,000. However, salaries can range from $30,000 to over $50,000, depending on various factors.
Certified Professional Compliance Officer (CPCO)
Overview
The Certified Professional Compliance Officer (CPCO) certification is offered by the AAPC. This certification is designed for professionals who want to specialize in healthcare compliance and ensure that healthcare organizations adhere to legal and ethical standards. CPCO-certified professionals play a vital role in preventing fraud, promoting compliance, and mitigating risks within the healthcare industry.
Requirements
To become a Certified Professional Compliance Officer (CPCO), you need to meet certain requirements set by the AAPC. These requirements include a high school diploma or equivalent and at least two years of experience working in a compliance-related role in healthcare. Additionally, you must also have a good understanding of healthcare laws, regulations, and industry standards.
Exam
To obtain the CPCO certification, you must pass the CPCO exam. This exam assesses your knowledge and skills in healthcare compliance, fraud prevention, and risk management. The exam consists of multiple-choice questions and covers various topics related to healthcare compliance. It is essential to study compliance regulations and practice scenario-based questions to prepare effectively for the exam.
Job Prospects
Having a CPCO certification can provide you with numerous job opportunities in healthcare compliance. CPCO-certified professionals can work in hospitals, healthcare consulting firms, government agencies, insurance companies, and other healthcare organizations. With the increasing focus on compliance and risk management in healthcare, the demand for CPCO-certified professionals is expected to grow.
Salary
The salary for CPCO-certified professionals can vary based on factors such as experience, location, and job role. On average, CPCO-certified compliance officers earn a competitive salary that reflects their specialized skills in healthcare compliance. According to the AAPC’s Salary Survey, the average annual salary for CPCO-certified professionals is around $70,000. However, salaries can range from $50,000 to over $90,000, depending on various factors.
Certified Outpatient Coder (COC)
Overview
The Certified Outpatient Coder (COC) certification is offered by the AAPC. This certification is suitable for individuals who want to specialize in outpatient coding and have a good understanding of outpatient procedures and services. COC-certified professionals play a crucial role in accurately coding and documenting outpatient medical records for reimbursement purposes.
Requirements
To become a Certified Outpatient Coder (COC), you need to meet certain requirements set by the AAPC. These requirements include a high school diploma or equivalent and a good understanding of medical terminology, anatomy, and outpatient-specific coding guidelines. Additionally, you must also have at least two years of coding experience in an outpatient setting or complete an AAPC-approved outpatient coding program.
Exam
To obtain the COC certification, you must pass the COC exam. This exam assesses your knowledge and skills in outpatient coding, CPT coding guidelines, and compliance regulations. The exam consists of multiple-choice questions and requires a thorough understanding of outpatient coding scenarios. It is essential to study coding guidelines and practice outpatient coding scenarios to prepare effectively for the exam.
Job Prospects
Having a COC certification can provide you with various job opportunities in outpatient coding. COC-certified professionals can work in outpatient clinics, ambulatory surgical centers, rehabilitation facilities, and other outpatient healthcare settings. The demand for COC-certified coders is expected to grow as outpatient procedures continue to increase.
Salary
The salary for COC-certified professionals can vary based on factors such as experience, location, and job role. On average, COC-certified coders earn a competitive salary that reflects their specialized skills in outpatient coding. According to the AAPC’s Salary Survey, the average annual salary for certified outpatient coders is around $57,000. However, salaries can range from $45,000 to over $70,000, depending on various factors.
Certified Inpatient Coder (CIC)
Overview
The Certified Inpatient Coder (CIC) certification is offered by the AAPC. This certification is suitable for individuals who want to specialize in inpatient coding and have a deep understanding of inpatient procedures, diagnoses, and coding guidelines. CIC-certified professionals play a crucial role in accurately coding and documenting inpatient medical records for reimbursement purposes.
Requirements
To become a Certified Inpatient Coder (CIC), you need to meet certain requirements set by the AAPC. These requirements include a high school diploma or equivalent and a good understanding of medical terminology, anatomy, and inpatient-specific coding guidelines. Additionally, you must also have at least two years of coding experience in an inpatient setting or complete an AAPC-approved inpatient coding program.
Exam
To obtain the CIC certification, you must pass the CIC exam. This exam assesses your knowledge and skills in inpatient coding, ICD coding guidelines, and compliance regulations. The exam consists of multiple-choice questions and requires a thorough understanding of inpatient coding scenarios. It is essential to study coding guidelines and practice inpatient coding scenarios to prepare effectively for the exam.
Job Prospects
Having a CIC certification can provide you with various job opportunities in inpatient coding. CIC-certified professionals can work in hospitals, rehabilitation centers, long-term care facilities, and other inpatient healthcare settings. The demand for CIC-certified coders is expected to grow as the complexity of inpatient coding and billing increases.
Salary
The salary for CIC-certified professionals can vary based on factors such as experience, location, and job role. On average, CIC-certified coders earn a competitive salary that reflects their specialized skills in inpatient coding. According to the AAPC’s Salary Survey, the average annual salary for certified inpatient coders is around $62,000. However, salaries can range from $50,000 to over $75,000, depending on various factors.
Certified Professional Medical Auditor (CPMA)
Overview
The Certified Professional Medical Auditor (CPMA) certification is offered by the AAPC. This certification is suitable for professionals who want to specialize in medical auditing and ensure compliance with coding and billing guidelines. CPMA-certified professionals play a crucial role in conducting audits, identifying errors or discrepancies, and making recommendations for improved coding and billing practices.
Requirements
To become a Certified Professional Medical Auditor (CPMA), you need to meet certain requirements set by the AAPC. These requirements include a high school diploma or equivalent and a strong understanding of medical coding, billing, and compliance regulations. Additionally, you must also have at least two years of experience in medical auditing or complete an AAPC-approved auditing program.
Exam
To obtain the CPMA certification, you must pass the CPMA exam. This exam assesses your knowledge and skills in medical auditing, compliance regulations, and healthcare documentation. The exam consists of multiple-choice questions and requires a thorough understanding of auditing principles and practices. It is essential to study auditing guidelines and practice auditing scenarios to prepare effectively for the exam.
Job Prospects
Having a CPMA certification can provide you with various job opportunities in medical auditing. CPMA-certified professionals can work in hospitals, insurance companies, consulting firms, government agencies, and other healthcare organizations. The demand for CPMA-certified auditors is expected to grow as the focus on auditing and compliance in healthcare continues to increase.
Salary
The salary for CPMA-certified professionals can vary based on factors such as experience, location, and job role. On average, CPMA-certified auditors earn a competitive salary that reflects their specialized skills in medical auditing. According to the AAPC’s Salary Survey, the average annual salary for certified medical auditors is around $70,000. However, salaries can range from $50,000 to over $90,000, depending on various factors.
Certified Physician Practice Manager (CPPM)
Overview
The Certified Physician Practice Manager (CPPM) certification is offered by the AAPC. This certification is suitable for professionals who want to specialize in managing the operations of physician practices. CPPM-certified professionals play a crucial role in ensuring the effective and efficient management of medical offices, including financial management, human resources, and compliance with healthcare regulations.
Requirements
To become a Certified Physician Practice Manager (CPPM), you need to meet certain requirements set by the AAPC. These requirements include a high school diploma or equivalent and a good understanding of medical practice management principles, healthcare regulations, and coding and billing guidelines. Additionally, you must also have at least two years of experience in healthcare management or complete an AAPC-approved practice management program.
Exam
To obtain the CPPM certification, you must pass the CPPM exam. This exam assesses your knowledge and skills in medical practice management, financial management, human resources, and compliance regulations. The exam consists of multiple-choice questions and requires a thorough understanding of practice management principles. It is essential to study management guidelines and practice scenario-based questions to prepare effectively for the exam.
Job Prospects
Having a CPPM certification can provide you with various job opportunities in physician practice management. CPPM-certified professionals can work in private physician practices, healthcare consulting firms, hospitals, and other healthcare organizations. With the increasing complexity of healthcare regulations and financial management in physician practices, the demand for CPPM-certified professionals is expected to grow.
Salary
The salary for CPPM-certified professionals can vary based on factors such as experience, location, and job role. On average, CPPM-certified practice managers earn a competitive salary that reflects their specialized skills in medical practice management. According to the AAPC’s Salary Survey, the average annual salary for certified physician practice managers is around $80,000. However, salaries can range from $60,000 to over $100,000, depending on various factors.
Certified Risk Adjustment Coder (CRC)
Overview
The Certified Risk Adjustment Coder (CRC) certification is offered by the AAPC. This certification is suitable for professionals who want to specialize in risk adjustment coding and ensure accurate reimbursement for Medicare Advantage and other risk-based payment models. CRC-certified professionals play a crucial role in identifying and documenting chronic conditions and other factors that affect patient risk scores.
Requirements
To become a Certified Risk Adjustment Coder (CRC), you need to meet certain requirements set by the AAPC. These requirements include a high school diploma or equivalent and a good understanding of risk adjustment coding guidelines, healthcare regulations, and documentation practices. Additionally, you must also have at least two years of coding experience in risk adjustment or complete an AAPC-approved risk adjustment coding program.
Exam
To obtain the CRC certification, you must pass the CRC exam. This exam assesses your knowledge and skills in risk adjustment coding principles, reimbursement methodologies, and compliance regulations. The exam consists of multiple-choice questions and requires a thorough understanding of risk adjustment coding scenarios. It is essential to study coding guidelines and practice risk adjustment coding scenarios to prepare effectively for the exam.
Job Prospects
Having a CRC certification can provide you with various job opportunities in risk adjustment coding. CRC-certified professionals can work in healthcare organizations that participate in Medicare Advantage and other risk-based payment models. With the increasing emphasis on accurate documentation and coding to reflect the severity of patient conditions, the demand for CRC-certified professionals is expected to grow.
Salary
The salary for CRC-certified professionals can vary based on factors such as experience, location, and job role. On average, CRC-certified coders earn a competitive salary that reflects their specialized skills in risk adjustment coding. According to the AAPC’s Salary Survey, the average annual salary for certified risk adjustment coders is around $60,000. However, salaries can range from $45,000 to over $75,000, depending on various factors.
In conclusion, there are several certifications available for individuals looking to enter the field of medical billing and coding. Each certification focuses on different aspects of coding, billing, compliance, or practice management. The Certified Professional Coder (CPC) and Certified Coding Specialist (CCS) certifications are well-recognized in the industry and offer opportunities for specialization in various healthcare settings. The Certified Professional Biller (CPB) certification is ideal for individuals looking to specialize in medical billing, while the Certified Coding Associate (CCA) certification serves as an entry-level certification for coding professionals. The Certified Professional Compliance Officer (CPCO) certification is suitable for professionals involved in healthcare compliance, and the Certified Outpatient Coder (COC) and Certified Inpatient Coder (CIC) certifications focus on outpatient and inpatient coding, respectively. The Certified Professional Medical Auditor (CPMA) certification is for those interested in medical auditing, while the Certified Physician Practice Manager (CPPM) certification is for individuals aspiring to manage physician practices. Lastly, the Certified Risk Adjustment Coder (CRC) certification is designed for professionals involved in risk adjustment coding for Medicare Advantage and other risk-based payment models. These certifications provide individuals with the knowledge, skills, and credentials necessary to succeed in the dynamic field of medical billing and coding.
Clinical coding plays a crucial role in the healthcare industry by translating medical diagnoses, procedures, and other healthcare services into a standardized language. Ensuring accuracy and consistency, clinical coding allows for effective communication and streamlined data management, facilitating proper patient care, billing, and research. By converting complex medical information into a structured code system, clinical coding contributes to a more efficient healthcare system and helps healthcare professionals make informed decisions based on accurate and comprehensive data.
Overview of Clinical Coding
Definition of Clinical Coding
Clinical coding is a crucial process in the healthcare industry that involves the translation of medical diagnoses, procedures, and resources into alphanumeric codes. These codes are used to classify and document patient encounters, facilitate efficient billing and reimbursement, support healthcare research and statistics, and ensure accurate medical documentation. By assigning specific codes to medical information, clinical coding plays a significant role in standardizing healthcare data.
Importance of Clinical Coding
Clinical coding is vital for several reasons. Firstly, it ensures that medical documentation is accurate and consistent, allowing healthcare professionals to communicate effectively and make informed decisions about patient care. Additionally, clinical coding facilitates efficient billing and reimbursement processes, enabling healthcare organizations to receive timely and appropriate payments for the services they provide. Moreover, it supports healthcare research and statistics, allowing for the analysis of trends, treatment outcomes, and the effectiveness of interventions.
Role of Clinical Coding in Healthcare
Ensure Accurate Medical Documentation
Clinical coding plays a pivotal role in ensuring accurate medical documentation. By assigning specific codes to diagnoses, procedures, and resources, clinical coders contribute to the standardization and consistency of health records. This standardized documentation not only aids in the effective communication of patient information among healthcare providers but also supports clinical decision-making and ensures continuity of care across different settings and providers.
Facilitate Efficient Billing and Reimbursement
Efficient billing and reimbursement are essential for the financial sustainability of healthcare organizations. Clinical coding enables accurate and timely billing by translating complex medical information into codes that represent the services provided. These codes are then used for claims submission to insurance companies or government reimbursement programs. By ensuring coding accuracy, clinical coders help healthcare organizations receive appropriate payments for their services and minimize the risk of claims rejection or denial.
Support Healthcare Research and Statistics
Clinical coding is a valuable tool for healthcare research and the generation of statistics. By coding medical information consistently and accurately, clinical coders create a standardized dataset that can be analyzed to identify patterns, trends, and outcomes. This data is essential for conducting epidemiological studies, monitoring population health, evaluating the effectiveness of interventions, and identifying areas for improvement in healthcare delivery. Accurate clinical coding contributes to the reliability and validity of research findings and helps inform evidence-based practice.
Clinical Coding Systems
International Classification of Diseases (ICD)
The International Classification of Diseases (ICD) is a globally recognized coding system used to classify and code diseases, injuries, and other health conditions. It provides a standardized framework for capturing and documenting medical information and supports the consistent reporting of diagnoses across healthcare settings. The latest version, ICD-10, is widely adopted and allows for greater specificity in coding. The upcoming transition to ICD-11 will bring further improvements in capturing healthcare data and enhancing clinical coding accuracy.
Current Procedural Terminology (CPT)
The Current Procedural Terminology (CPT) is a coding system developed by the American Medical Association to describe medical procedures and services provided by healthcare professionals. CPT codes are used for billing and reimbursement purposes in the United States. They provide a standardized language for describing medical procedures and services, allowing for the accurate and efficient communication of information between healthcare providers, payers, and regulatory bodies.
Healthcare Common Procedure Coding System (HCPCS)
The Healthcare Common Procedure Coding System (HCPCS) is another coding system used in the United States to describe and identify healthcare services, supplies, and equipment. HCPCS codes are used for billing and reimbursement purposes, particularly for services not covered by CPT codes. The system includes two levels of codes – Level I (which is the CPT codes) and Level II (which includes codes for items such as durable medical equipment, prosthetics, and supplies).
Clinical Coding Process
Patient Encounter and Documentation
The clinical coding process begins with the patient encounter and documentation of medical information. Healthcare professionals document the patient’s medical history, symptoms, diagnoses, procedures performed, and other relevant details. Accurate and comprehensive documentation is essential to ensure that all relevant information is captured and that clinical coders can assign the appropriate codes based on the medical record.
Code Assignment and Selection
Once the patient’s information is documented, clinical coders analyze the medical record and assign the appropriate codes based on established coding guidelines. They identify and code the patient’s diagnoses, procedures, and resources used during the encounter. This process involves a deep understanding of coding systems, medical terminology, and coding guidelines to ensure accuracy and compliance with industry standards.
Quality Assurance and Compliance
To ensure coding accuracy, healthcare organizations implement quality assurance measures through regular audits and reviews. This includes assessing the accuracy and completeness of coded data, ensuring compliance with coding guidelines and regulations, and identifying areas for improvement and training. Internal and external coding audits help maintain the integrity of clinical coding and support accurate medical documentation, efficient billing, and reimbursement processes, and reliable healthcare statistics.
Roles and Responsibilities of Clinical Coders
This image is property of fabnhsstuff.net.
Certification and Education Requirements
Clinical coders are highly skilled professionals who undergo specialized training and certification. They typically hold certifications such as Certified Coding Specialist (CCS) or Certified Professional Coder (CPC) that validate their competence in clinical coding. These certifications require a comprehensive understanding of coding systems, medical terminology, anatomy, physiology, and disease processes. Continuous education is crucial for clinical coders to stay updated with evolving coding guidelines, regulations, and technological advancements.
Coding Accuracy and Efficiency
Clinical coders are responsible for accurately translating medical information into codes. They must possess strong analytical skills and attention to detail to ensure coding accuracy and compliance with coding guidelines. Alongside accuracy, clinical coders must also maintain efficiency in their coding processes to meet the demands of healthcare settings. Timely and accurate coding plays a crucial role in revenue cycle management by facilitating timely billing and reimbursement and reducing the risk of claims rejection or denial.
Collaboration with Healthcare Providers
Clinical coders collaborate closely with healthcare providers, including physicians, nurses, and other allied health professionals. They work together to ensure accurate and complete documentation of patient encounters, clarify clinical details, and address any coding-related queries. Effective communication and collaboration enhance coding accuracy and enable healthcare providers to receive appropriate reimbursement for the services they provide.
Clinical Coding and Revenue Cycle Management
Support for Medical Billing
Clinical coding is a fundamental part of the revenue cycle management process in healthcare organizations. Accurate clinical coding enables the generation of claims for medical services provided to patients. These claims are then submitted to insurance companies or government reimbursement programs for payment. Without proper clinical coding, healthcare organizations would struggle to receive timely and appropriate payment for the care they deliver.
Documentation Improvement
Clinical coding plays a crucial role in documentation improvement initiatives within healthcare organizations. By ensuring accurate and detailed coding, clinical coders contribute to the completeness and specificity of medical records. This improves the accuracy of clinical documentation, supports effective communication among healthcare providers, and reduces the risk of coding-related errors. Enhanced documentation also facilitates better coordination of care, improves patient safety, and ensures the continuity of care across different healthcare settings.
Financial Impact on Healthcare Organizations
Accurate clinical coding has a direct financial impact on healthcare organizations. Coding errors or omissions can lead to claims rejection or denial, resulting in delayed or lost revenue for healthcare providers. Moreover, inaccurate coding can result in overpayment or underpayment for services rendered, affecting the financial viability of the organization. By ensuring coding accuracy and compliance, clinical coders contribute to the financial health and sustainability of healthcare organizations.
Importance of Coding Accuracy
Claims Rejection and Denials
Coding accuracy is crucial to prevent claims rejection or denial by insurance companies or government reimbursement programs. Inaccurate or incomplete coding can result in rejected or delayed claims, leading to delayed payments for healthcare services and potential financial difficulties for healthcare organizations. By ensuring coding accuracy and compliance with coding guidelines, clinical coders minimize the risk of claims rejection or denial, resulting in a smoother and more efficient revenue cycle.
Clinical Decision Making
Accurate coding has a direct impact on clinical decision-making. When evaluating patient records, healthcare providers rely on coded data to understand the patient’s medical history, diagnoses, and procedures performed. Inaccurate or incomplete coding can lead to wrong interpretations and incorrect clinical decisions, potentially compromising patient care and outcomes. By maintaining coding accuracy, clinical coders contribute to the reliability and quality of clinical decision-making, allowing for informed and evidence-based patient care.
Patient Safety and Quality of Care
Coding accuracy also plays a significant role in patient safety and the overall quality of care provided. Accurate coding ensures that healthcare providers have a complete and precise understanding of a patient’s conditions, treatments, and interventions. This information is crucial for effective care coordination, medication management, and the prevention of medical errors. By accurately coding medical information, clinical coders contribute to patient safety, improved outcomes, and the overall quality of healthcare delivery.
Challenges in Clinical Coding
Complexity of Coding Guidelines
Clinical coding is a highly complex task that requires a deep understanding of coding systems and guidelines. The coding guidelines, such as those provided by the American Hospital Association (AHA) and the Centers for Medicare and Medicaid Services (CMS), are extensive and regularly updated to reflect changes in medical practice and technology. Clinical coders must continuously keep up with these evolving guidelines to ensure accurate coding and comply with regulatory requirements, presenting a constant challenge in the field.
Evolving Healthcare Regulations
Healthcare regulations and reimbursement policies undergo frequent changes, adding another layer of complexity to clinical coding. Clinical coders must stay updated on the latest regulatory changes, such as those introduced by the CMS or private insurance companies, to ensure compliance and accurate coding. These regulatory changes often aim to improve transparency, standardization, and fraud prevention in healthcare, but they can pose challenges for clinical coders as they navigate the ever-changing landscape.
Technological Advancements
While technology brings numerous advancements to the healthcare industry, it also poses challenges in clinical coding. The implementation of electronic health records (EHRs) has transformed the way medical information is captured and stored. Clinical coders must adapt to new technologies and software systems, ensuring they are proficient in using EHRs and other coding tools. Additionally, the increasing use of artificial intelligence and machine learning in coding processes requires clinical coders to develop new skills and embrace the capabilities of technology to enhance coding accuracy and efficiency.
Emerging Trends in Clinical Coding
This image is property of static.wixstatic.com.
Implementation of Electronic Health Records (EHR)
The implementation of electronic health records (EHRs) has revolutionized the way healthcare organizations capture, store, and share patient information. EHRs provide clinical coders with immediate access to patient records, streamlining the coding process and enhancing accuracy. The integration of coding tools within EHR systems facilitates real-time coding, reduces administrative burden, and improves coding efficiency. The ongoing advancement in EHR technology presents exciting opportunities to further automate and optimize clinical coding processes.
Artificial Intelligence and Machine Learning
The field of clinical coding is experiencing transformative advancements with the integration of artificial intelligence (AI) and machine learning (ML) algorithms. AI-powered coding tools are being developed to automate code assignment and increase coding accuracy. ML algorithms analyze vast amounts of data, identify patterns, and suggest appropriate codes based on historical coding decisions. These technological advancements have the potential to revolutionize clinical coding, improving coding accuracy, efficiency, and productivity.
Remote and Virtual Coding
Another emerging trend in clinical coding is the adoption of remote and virtual coding. Remote coding allows clinical coders to work from home or off-site locations, offering flexibility and cost savings for healthcare organizations. Virtual coding involves the use of secure software and communication tools to assign codes remotely, facilitating collaboration and minimizing the need for physical infrastructure. Remote and virtual coding options are particularly valuable during times of crisis, such as the COVID-19 pandemic, when remote work has become more prevalent.
Future of Clinical Coding
Automation and Integration
The future of clinical coding lies in automation and integration. As technology continues to advance, clinical coding processes will become increasingly automated. AI-powered coding algorithms will assist clinical coders in assigning codes accurately and efficiently, reducing the risk of human error. Integration of coding tools within EHR systems will streamline coding processes, enabling real-time coding and seamless sharing of information between healthcare providers, coders, and billing departments.
Interoperability with Healthcare Systems
Interoperability is a critical aspect of the future of clinical coding. As healthcare systems become more integrated, the exchange of coded information will become seamless across different settings and platforms. Shared electronic health records and interoperable coding systems will improve care coordination, enhance data accuracy, and reduce administrative burden. The ability to exchange coded information across healthcare providers and organizations will contribute to a comprehensive and holistic understanding of patient health.
Continued Education and Professional Development
Continuous education and professional development will be essential for clinical coders in the future. As coding guidelines, regulations, and technology evolve, clinical coders must stay updated and enhance their skills and knowledge. Ongoing education and training programs will ensure that clinical coders remain proficient in coding systems, medical terminology, and emerging technologies. By investing in the professional development of clinical coders, healthcare organizations can ensure the accuracy and reliability of clinical coding processes.
In conclusion, clinical coding plays a vital role in the healthcare industry, ensuring accurate medical documentation, facilitating efficient billing and reimbursement, and supporting healthcare research and statistics. Clinical coders have the responsibility of assigning codes accurately, complying with coding guidelines, and collaborating with healthcare providers. Challenges in clinical coding, such as the complexity of coding guidelines, evolving healthcare regulations, and technological advancements, need to be addressed through continuous education and staying updated with emerging trends. The future of clinical coding lies in automation, interoperability, and the continued professional development of clinical coders.
In the world of medical billing, modifiers play a crucial role in accurately documenting and coding procedures. Effective utilization of modifiers can significantly impact the reimbursement process and minimize coding errors. This article aims to shed light on the different types of modifiers used in medical billing, their purpose, and how they enhance the accuracy and transparency of healthcare claims. Understanding these modifiers is essential for healthcare providers and billing professionals to ensure precise coding, streamline the billing process, and optimize reimbursement rates.
Modifiers in Medical Billing
modifiers play a crucial role in the realm of medical billing. They serve as additional codes that can be appended to a healthcare service or procedure to provide further clarification or information to the payer. These modifiers help in accurately conveying the nature of the service provided, any special circumstances, or any variations from the usual billing practices. By understanding the definition, purpose, and importance of modifiers, healthcare professionals can ensure accurate and efficient reimbursement for the services they provide.
Definition of Modifiers
Modifiers are two-character alphanumeric codes that are added to the primary procedure code in medical billing. These codes help to modify the way a service or procedure is identified and reimbursed. Modifiers provide additional information about the service to the payer, such as the method, extent, or circumstances of the procedure. They allow healthcare providers to communicate any significant changes or variations that may impact the billing and coding process.
Purpose of Modifiers
The primary purpose of modifiers in medical billing is to provide additional information and clarification to the payer. These codes enable healthcare professionals to accurately describe the services they provide, ensuring that the submitted claims reflect the complex nature of the procedures performed. Modifiers serve to eliminate ambiguities and facilitate accurate billing by indicating any special circumstances or variations that may affect reimbursement. Additionally, modifiers help prevent claim denials, delays, or incorrect payments by providing the necessary context for the billed services.
Importance of Modifiers in Medical Billing
The importance of modifiers in medical billing cannot be overstated. Proper use of modifiers ensures accurate reimbursement for the services rendered by healthcare providers. By effectively communicating any special circumstances or variations, modifiers help to justify the need for specific services and facilitate proper payment from insurance payers. Moreover, modifiers help in fulfilling the requirements of insurance companies, maintaining compliance with billing regulations, and reducing the likelihood of billing errors or fraudulent claims. Overall, modifiers play a vital role in ensuring streamlined medical billing processes and improved financial outcomes for healthcare practitioners.
This image is property of www.veralon.com.
Types of Modifiers
Modifiers are classified into various categories based on the specific nature of the service or procedure. These categories include Evaluation and Management (E/M) modifiers, Anatomic modifiers, Global Surgery modifiers, Surgical modifiers, Radiology modifiers, Pathology and Laboratory modifiers, Durable Medical Equipment (DME) modifiers, Ambulance modifiers, Preventive Services modifiers, and Mental Health Services modifiers. Let’s explore each category in detail:
Evaluation and Management (E/M) Modifiers
Evaluation and Management modifiers are commonly used in medical billing to indicate specific circumstances or variations related to E/M services. These modifiers are added to the E/M codes to provide detailed information about the complexity, location, or other unique aspects of the service. For example, Modifier 25 is used to indicate that an E/M service was separately identifiable from a procedure performed on the same day.
Anatomic Modifiers
Anatomic modifiers are used to indicate a specific anatomical site upon which a procedure is performed. These modifiers help in specifying the exact location of the service, thereby providing additional details for proper reimbursement. An example of an anatomic modifier is Modifier F1, which indicates that a procedure was performed on the left hand.
Global Surgery Modifiers
Global Surgery modifiers are used to identify specific circumstances related to procedures with global surgical periods. These modifiers help in distinguishing between pre-operative, intra-operative, and post-operative services provided by the surgeon. Modifier 24 is an example of a global surgery modifier that indicates a separately identifiable evaluation and management service performed during the post-operative period.
Surgical Modifiers
Surgical modifiers are used to provide additional information about surgical procedures. These modifiers help in indicating specific circumstances or variations related to the surgical service provided. For instance, Modifier 51 indicates that multiple procedures were performed during the same surgical session.
Radiology Modifiers
Radiology modifiers are used to provide further details about radiological services or imaging studies. These modifiers help in indicating different aspects of the radiology service, such as the number of views, multiple procedures performed, or the use of specific equipment. An example is Modifier 26, which indicates that only the professional component of a radiological service was performed.
Pathology and Laboratory Modifiers
Pathology and Laboratory modifiers are used to provide details about laboratory services or diagnostic tests. These modifiers help in specifying circumstances that may impact the billing and coding of these services, such as site-specific or technical components. Modifier 90, for example, indicates that a laboratory test was performed outside the usual reference range.
Durable Medical Equipment (DME) Modifiers
Durable Medical Equipment modifiers are used to identify specific circumstances related to the use of durable medical equipment. These modifiers help in providing further details about the equipment used or any necessary accessories. An example of a DME modifier is Modifier RR, which indicates rental equipment.
Ambulance Modifiers
Ambulance modifiers are used to indicate specific circumstances related to ambulance services. These modifiers help in providing additional information about the transportation or level of service provided during an ambulance transport. Modifier RH, for instance, indicates that a physician was present during a medical emergency transport.
Preventive Services Modifiers
Preventive Services modifiers are used to identify specific circumstances related to preventive healthcare services. These modifiers help in indicating additional information about the preventive services provided or specific aspects related to preventive care. Modifier 33 is an example of a preventive services modifier that indicates a preventive service was performed.
Mental Health Services Modifiers
Mental Health Services modifiers are used to specify certain aspects of mental health services. These modifiers help in indicating details about the type of service provided or specific circumstances related to mental health care. Modifier GT, for example, indicates that telehealth services were provided for mental health care.
In conclusion, modifiers serve as vital components in medical billing, providing additional information and clarification to ensure accurate reimbursement for healthcare services. Understanding the different types of modifiers and their specific purposes enables healthcare professionals to effectively communicate the complexities of the services they provide. By utilizing modifiers correctly, healthcare providers can streamline their billing processes and ensure proper payment for the care they deliver.
In the field of healthcare, clinical codes play a crucial role in organizing and categorizing medical information. By assigning specific codes to different diagnoses, procedures, medications, and other healthcare components, these classification systems ensure consistency and facilitate accurate data management. In this article, we will explore the various types of clinical codes used in medical practice, examining their significance and providing examples to shed light on their practical applications.
This image is property of www.medicalcodingbuff.com.
Introduction
Clinical codes are essential tools used in healthcare to classify and categorize medical diagnoses, procedures, treatments, and substances. These codes serve as a common language for healthcare professionals, researchers, and insurance providers, ensuring accurate and standardized documentation of patient information. The use of clinical codes enables efficient healthcare management, billing, and research analysis. In this article, we will explore the different types of clinical codes and their significance in healthcare.
International Classification of Diseases (ICD)
The International Classification of Diseases (ICD) is the most widely used and internationally recognized clinical coding system. It provides a standardized framework for classifying diseases, injuries, and other health conditions. The ICD system is regularly updated to reflect advances in medical knowledge and capture evolving healthcare practices.
ICD-10-CM
ICD-10-CM (Clinical Modification) is the current version of the ICD classification system used in the United States. It consists of alphanumeric codes that represent different diseases, symptoms, and abnormal findings. The codes in ICD-10-CM provide a detailed description of a patient’s health condition, allowing healthcare professionals to accurately diagnose and treat various diseases.
ICD-10-PCS
ICD-10-PCS (Procedure Coding System) is another component of the ICD-10 classification. Unlike ICD-10-CM, which focuses on diagnoses, ICD-10-PCS is used to code medical procedures and interventions. This system enables the precise documentation of surgical procedures, making it valuable for surgical planning, billing, and statistical analysis.
ICD-11
ICD-11 is the upcoming revision of the International Classification of Diseases, which is expected to be implemented worldwide in the near future. ICD-11 incorporates significant changes, such as improved integration with electronic health records and an expanded range of diagnostic codes. This update aims to enhance the accuracy of clinical coding and provide a more comprehensive understanding of diseases and health conditions.
Current Procedural Terminology (CPT)
Current Procedural Terminology (CPT) is a coding system developed and maintained by the American Medical Association (AMA). It is widely used in the United States to report medical procedures and services to insurance companies for reimbursement purposes. CPT codes cover a broad range of medical specialties and are regularly updated to reflect advancements in medical technology and procedures.
Evaluation and Management Codes
Evaluation and Management (E/M) codes are a subset of CPT codes that are used to document patient encounters, including office visits, hospital visits, consultations, and telemedicine services. E/M codes provide a structured approach to recording the complexity and nature of the medical encounter, facilitating accurate reimbursement and reflecting the level of medical decision-making involved.
Anesthesia Codes
Anesthesia codes in the CPT system are used to classify different types and levels of anesthesia administered during surgical procedures. These codes consider factors such as the patient’s age, health status, and the procedure’s complexity to accurately represent the anesthesia services provided.
Surgery Codes
CPT surgery codes enable the precise documentation of surgical procedures, including both invasive and non-invasive techniques. These codes provide detailed descriptions of specific surgeries, facilitating accurate billing, tracking surgical outcomes, and supporting research and analysis.
Radiology Codes
Radiology codes in the CPT system cover a wide range of diagnostic imaging procedures, such as X-rays, CT scans, MRIs, and ultrasounds. These codes capture the specific type of imaging procedure performed, the body part examined, and the complexity of the test, ensuring accurate reimbursement and tracking of imaging services.
Pathology and Laboratory Codes
Pathology and Laboratory codes in the CPT system are used to classify laboratory tests, pathology procedures, and other diagnostic services. These codes capture the specific test performed, the specimen type, and the methodology used, enabling accurate billing and analysis of laboratory services.
Medicine Codes
Medicine codes in the CPT system encompass a broad range of services, such as non-surgical treatments, vaccinations, and administration of medications. These codes provide a standardized way of documenting medical services not covered by other CPT code categories, ensuring accurate reimbursement and tracking of medical treatments.
Healthcare Common Procedure Coding System (HCPCS)
The Healthcare Common Procedure Coding System (HCPCS) is a coding system used in the United States to identify and categorize medical services, supplies, and equipment not covered by CPT codes. HCPCS is divided into two levels: Level I and Level II.
Level I HCPCS Codes
Level I HCPCS codes comprise the subset of CPT codes used to report services provided by physicians, non-physician practitioners, and medical facilities. These codes are integrated into the broader HCPCS system and are primarily used for billing and reimbursement purposes.
Level II HCPCS Codes
Level II HCPCS codes cover a wide range of medical supplies, durable medical equipment, and other healthcare services not included in CPT codes. These codes are used by non-physician providers, such as ambulance services, home healthcare agencies, and medical suppliers, to accurately document and bill for their services.
SNOMED CT
SNOMED CT (Systematized Nomenclature of Medicine – Clinical Terms) is a comprehensive clinical coding system used globally to support the electronic exchange of clinical health information. It consists of a vast collection of medical concepts, their descriptions, and relationships, providing a standardized terminology for clinical documentation and data exchange.
Concepts
SNOMED CT includes a broad range of concepts representing various diseases, procedures, symptoms, anatomical structures, and substances. Each concept is assigned a unique code and standardized name, enabling precise and consistent communication across healthcare systems and settings.
Description Logic
SNOMED CT incorporates description logic, a formal logic system, to support advanced reasoning capabilities and semantic precision. This allows healthcare professionals and computer systems to accurately interpret and analyze the meaning of coded clinical information, enhancing the accuracy and interoperability of healthcare data.
Relationships
SNOMED CT facilitates the representation of complex relationships between different clinical concepts. These relationships capture various aspects, such as anatomical structure hierarchies, disease classifications, and procedures’ dependencies, enabling more comprehensive and nuanced clinical documentation, research, and analysis.
Logical Observation Identifiers Names and Codes (LOINC)
The Logical Observation Identifiers Names and Codes (LOINC) is a widely used coding system for identifying laboratory and clinical observations. LOINC codes enable the standardization and interoperability of laboratory and clinical data, allowing healthcare professionals and researchers to compare and analyze results across different healthcare organizations and systems.
Universal Code System
LOINC provides a universal code system for identifying and exchanging laboratory and clinical observations, such as laboratory tests, vital signs, and clinical assessments. These codes ensure consistency and comparability in documenting and sharing patient information, supporting improved patient care and research outcomes.
Component and Property
LOINC codes consist of two main components: a component code and a property code. The component code represents the type of observation, while the property code defines the specific characteristic being measured or observed. This dual-component structure enables precise identification and classification of a wide range of laboratory and clinical observations.
Units of Measure
LOINC codes also include standard units of measure for laboratory and clinical observations. These units provide a consistent and unambiguous representation of measurement values, facilitating accurate interpretation and comparison of data across different healthcare systems and settings.
This image is property of cdn.sketchbubble.com.
RxNorm
RxNorm is a standardized terminology and drug vocabulary developed by the National Library of Medicine in the United States. It encompasses a comprehensive collection of medication-related concepts, facilitating the exchange of medication information and supporting medication management across different healthcare systems.
Unique Ingredient Identifier (UNII)
RxNorm incorporates the Unique Ingredient Identifier (UNII) system, which assigns a unique code to each active ingredient found in medication products. This enables precise identification and linkage of medication ingredients, supporting accurate medication management, adverse event reporting, and medication reconciliation.
Prescribable Names
RxNorm includes prescribable names for medication products, representing the names used in clinical practice when prescribing medications. These names align with national drug formularies, product monographs, and drug compendia, ensuring consistent and standardized medication prescribing across healthcare settings.
Semantic Clinical Drugs
RxNorm’s Semantic Clinical Drugs (SCD) subset provides a refined representation of medication concepts, focusing on clinically relevant drug information. SCD concepts encompass aspects such as drug ingredients, strengths, dosage forms, and routes of administration, enabling accurate and precise medication documentation, analysis, and decision support.
Current Dental Terminology (CDT)
Current Dental Terminology (CDT) is a coding system developed by the American Dental Association (ADA) to document dental procedures and services. CDT codes provide a standardized approach to dental coding, facilitating accurate billing, communication, and analysis of dental treatments.
Veterinary Classification of Procedures (VetCPT)
Veterinary Classification of Procedures (VetCPT) is a coding system used in veterinary medicine to classify and document veterinary procedures and services. VetCPT codes provide a structured framework for veterinary coding, allowing for accurate billing, tracking of veterinary treatments, and analysis of animal health outcomes.
Conclusion
Clinical codes play a pivotal role in healthcare by providing a standardized language for classifying medical diagnoses, procedures, treatments, and substances. The various coding systems, such as ICD, CPT, HCPCS, SNOMED CT, LOINC, RxNorm, CDT, and VetCPT, enable healthcare professionals, researchers, and insurance providers to accurately capture and communicate vital healthcare information. These codes facilitate efficient healthcare management, billing, research analysis, and interoperability, ultimately leading to improved patient care and outcomes. By understanding the different types of clinical codes and their significance, healthcare professionals can effectively utilize these coding systems to enhance healthcare delivery and advance medical knowledge.
In the field of medical billing, understanding the various types of plans is essential for accurately processing patients’ claims. This article explores the different types of plans commonly encountered in medical billing, covering insurance plans such as Health Maintenance Organizations (HMOs), Preferred Provider Organizations (PPOs), Point of Service (POS) plans, and Medicare/Medicaid. By gaining insight into these plans, you will be better equipped to navigate the complexities of medical billing and ensure proper reimbursement for healthcare services provided.
Types of Plans in Medical Billing
Medical billing is an essential part of the healthcare system, ensuring that healthcare providers receive payment for the services they render to patients. Within the realm of medical billing, there are various types of plans that individuals may have, each with its own set of rules and requirements. In this article, we will explore the different types of plans in medical billing, their features, and how they impact both healthcare providers and patients.
Private Insurance Plans
Private insurance plans are typically obtained through an employer or purchased individually. These plans are provided by private companies and offer a range of coverage options depending on the policy selected. Private insurance plans often have a network of preferred healthcare providers, commonly known as in-network providers. When seeking medical services from in-network providers, the plan usually covers a larger portion of the cost, while visiting out-of-network providers may result in higher out-of-pocket expenses.
Government Sponsored Plans
Government-sponsored plans are designed to provide healthcare coverage for specific segments of the population. The most well-known government-sponsored plans in the United States are Medicare and Medicaid. Medicare is available to individuals aged 65 and older, as well as those with certain disabilities. Medicaid, on the other hand, is a joint federal and state program that provides healthcare coverage for low-income individuals and families. These plans have specific guidelines and requirements for eligibility and coverage, and medical billing for government-sponsored plans follows unique processes..
Health Maintenance Organization (HMO) Plans
HMO plans are a type of managed care plan that focuses on preventive care and cost control. Under an HMO plan, individuals must select a primary care physician (PCP) who serves as the main point of contact for all healthcare needs. PCPs coordinate care and refer patients to specialists or hospitals within the HMO network. HMO plans typically require individuals to obtain a referral from their PCP before seeking specialized care. This system aims to control costs by directing individuals to specific providers and ensuring a coordinated approach to care.
Preferred Provider Organization (PPO) Plans
PPO plans, also known as managed care plans, offer a larger degree of flexibility compared to HMO plans. These plans allow individuals to seek care from both in-network and out-of-network providers. While individuals can see any healthcare provider they choose, visiting in-network providers typically results in lower out-of-pocket costs due to negotiated rates. PPO plans do not require individuals to obtain a referral before seeing a specialist, providing greater freedom and convenience in accessing healthcare services.
This image is property of i.ytimg.com.
Exclusive Provider Organization (EPO) Plans
EPO plans combine characteristics of both HMO and PPO plans. Similar to HMO plans, EPO plans require individuals to select a primary care physician and obtain referrals for specialized care within the network. However, like PPO plans, EPO plans do not cover services rendered by out-of-network providers, except in cases of emergencies. EPO plans aim to strike a balance between cost control and flexibility, ensuring that individuals receive coordinated care while still having the option to seek specialized services.
Point of Service (POS) Plans
POS plans are a hybrid of HMO and PPO plans, combining aspects of both. Individuals under a POS plan are required to select a primary care physician and obtain referrals for specialist care within the network. However, individuals also have the option to seek care outside the network without a referral, although this usually results in higher out-of-pocket costs. POS plans offer greater flexibility than HMO plans while still maintaining some cost control measures.
This image is property of www.altexsoft.com.
Fee-for-Service (FFS) Plans
Fee-for-Service plans, also known as traditional indemnity plans, provide the highest level of freedom when it comes to healthcare provider choice. Under an FFS plan, individuals can see any provider they want without the need for referrals. However, this freedom comes at a cost, as FFS plans often have higher premiums and deductibles compared to other types of plans. Additionally, individuals may need to submit claims themselves to receive reimbursement for covered services. FFS plans can be attractive for individuals who prioritize provider choice and are willing to pay higher costs.
High Deductible Health Plans (HDHP)
High Deductible Health Plans (HDHPs) are designed to lower monthly premiums in exchange for higher out-of-pocket costs. These plans feature a higher deductible than other types of plans, meaning individuals must pay a certain amount out of their own pocket before the insurance coverage kicks in. HDHPs are often paired with Health Savings Accounts (HSAs), which allow individuals to save pre-tax dollars to pay for qualified medical expenses. These plans can be a cost-effective option for individuals who are generally healthy and do not anticipate regular high-cost medical services.
This image is property of m.foolcdn.com.
Medicare Advantage Plans
Medicare Advantage plans, also known as Medicare Part C, are offered by private insurance companies approved by Medicare. These plans combine the benefits of Original Medicare (Part A and B) with additional coverage options, such as prescription drug coverage (Part D) and sometimes even additional benefits like dental or vision care. Medicare Advantage plans may have different rules and costs compared to Original Medicare, and individuals must continue paying their Medicare Part B premium in addition to any premium associated with the Medicare Advantage plan.
Medicaid and State Programs
Medicaid is a government-sponsored program that provides healthcare coverage for low-income individuals and families. Each state has its own Medicaid program, and eligibility requirements and coverage options may vary. Medicaid covers a wide array of medical services, including doctor visits, hospital stays, and prescription medications, among others. Enrollment in Medicaid is based on income and other factors, and individuals must meet certain criteria to qualify. State programs may also offer additional healthcare coverage options or assistance programs that complement Medicaid benefits.
In conclusion, understanding the different types of plans in medical billing is crucial for both healthcare providers and patients. The variety of plans available offers individuals the flexibility to choose the type of coverage that suits their needs and preferences. Healthcare providers must be well-versed in the intricacies of each plan to ensure accurate and timely billing, while patients must familiarize themselves with the specific guidelines, requirements, and costs associated with their chosen plan. By navigating the complex landscape of medical billing plans effectively, both healthcare providers and patients can work together to ensure quality care while maintaining financial stability.
In the field of healthcare, medical coding plays a vital role in ensuring accurate documentation and proper reimbursement for services rendered. It involves the assignment of alphanumeric codes to various medical procedures, diagnoses, and treatments. This article will explore a few notable examples of medical coding, highlighting its significance in healthcare management and the impact it has on both patients and healthcare providers alike. From the classification of diseases to the identification of specific pharmaceutical products, medical coding offers a systematic approach to streamline healthcare operations and facilitate effective communication among healthcare professionals.
Medical Coding Basics
Introduction to Medical Coding
Medical coding is an integral part of the healthcare industry as it plays a crucial role in the accurate documentation, billing, and reimbursement processes. It involves translating medical diagnoses, procedures, and services into alphanumeric codes, which are then used for communication and reimbursement purposes. This standardized system allows healthcare providers, insurance companies, and regulatory bodies to understand and track the services provided to patients.
Purpose of Medical Coding
The primary purpose of medical coding is to ensure uniformity and accuracy in healthcare documentation and billing processes. By assigning specific codes to medical diagnoses, procedures, and services, medical coding enables effective communication and information exchange between healthcare professionals, insurance companies, and other stakeholders. These codes also play a crucial role in determining appropriate reimbursement for healthcare services, facilitating research, and supporting quality improvement initiatives.
Medical Coding Systems
Medical coding systems form the foundation of the coding process, providing a structured framework for assigning codes to various healthcare services. The three main coding systems used in medical coding are:
International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM)
Current Procedural Terminology (CPT) Codes
Healthcare Common Procedure Coding System (HCPCS) Codes
ICD-10-CM
Overview of ICD-10-CM
ICD-10-CM is a widely used coding system designed to capture and classify diagnoses and signs, symptoms, abnormal findings, and external causes of diseases or injuries. It is maintained and regularly updated by the World Health Organization (WHO) and is used by healthcare providers, hospitals, and insurance companies globally. The system utilizes alphanumeric codes to categorize various medical conditions, providing a detailed and comprehensive classification framework.
Benefits of ICD-10-CM Coding
The implementation of ICD-10-CM has brought several benefits to the healthcare industry. Some of the key advantages include:
Increased Specificity: ICD-10-CM offers a greater level of detail and specificity compared to its predecessor, ICD-9-CM. This enables more accurate reporting and improved clinical documentation, resulting in better healthcare planning, resource allocation, and epidemiological research.
Enhanced Reimbursement: The use of ICD-10-CM codes enables healthcare providers to accurately code and bill for services provided to patients. This helps minimize billing errors and ensures appropriate reimbursement, ultimately enhancing financial stability for healthcare organizations.
Improved Research and Analytics: The detailed nature of ICD-10-CM codes allows for better analysis of healthcare data, leading to improved research capabilities, identification of disease patterns, and monitoring of public health trends. This enables proactive healthcare interventions and evidence-based decision-making.
Examples of ICD-10-CM Codes
ICD-10-CM codes cover a wide range of medical conditions. Here are some examples of ICD-10-CM codes:
A09 – Infectious gastroenteritis and colitis, unspecified
S72.001A – Unspecified fracture of right femur, initial encounter for closed fracture
CPT Codes
Overview of CPT Codes
Current Procedural Terminology (CPT) codes are a set of standard codes maintained by the American Medical Association (AMA). They are primarily used to describe medical procedures and services provided by healthcare professionals, such as physicians, surgeons, and other allied healthcare providers. CPT codes provide a common language for reporting medical procedures, facilitating accurate billing, and improving communication within the healthcare system.
Common CPT Codes
CPT codes cover a wide range of medical procedures and services. Some common categories of CPT codes include:
Evaluation and Management (E&M): These codes are used to document and bill for patient encounters, such as office visits, hospital visits, and consultations.
Surgical Procedures: CPT codes for surgical procedures cover various specialties, including general surgery, orthopedics, cardiovascular surgery, and more.
Diagnostic Testing: CPT codes exist for a range of diagnostic tests, such as blood tests, imaging studies (X-rays, MRIs), and electrocardiograms (ECGs).
Therapy Services: Codes for therapy services encompass physical therapy, occupational therapy, speech therapy, and other rehabilitative treatments.
Examples of CPT Codes
Here are a few examples of CPT codes to provide a better understanding of their usage:
99213 – Established patient office visit, typically 15 minutes
64721 – Carpal tunnel release, with or without tenosynovectomy
58662 – Laparoscopy, surgical; with bilateral total pelvic lymphadenectomy and biopsy(ies) of uterine adnexa
36415 – Collection of venous blood by venipuncture
90837 – Psychotherapy, 60 minutes, for an individual in an outpatient setting
HCPCS Codes
Introduction to HCPCS Codes
The Healthcare Common Procedure Coding System (HCPCS) is a coding system used to report and bill for supplies, equipment, and services that are not covered by CPT codes. HCPCS codes are maintained by the Centers for Medicare and Medicaid Services (CMS) and are used primarily in the United States. These codes provide a comprehensive range of alphanumeric codes that cover durable medical equipment, drugs, ambulance services, and more.
Types of HCPCS Codes
HCPCS codes are divided into two main levels. Level I codes are identical to CPT codes and represent physician and other providers’ services. Level II codes, on the other hand, are alphanumeric and cover items and services not included in Level I codes. Level II codes are further subdivided into various sections, including:
A – Transportation, Medical and Surgical Supplies, Miscellaneous and Experimental
E – Durable Medical Equipment (DME)
J – Drugs administered other than oral method, chemotherapy drugs
Examples of HCPCS Codes
Here are a few examples of HCPCS codes across different sections:
The Diagnosis-Related Group (DRG) coding system is used primarily for categorizing and classifying inpatient hospital stays in the United States. DRGs group patients with similar characteristics, conditions, and resource utilization, allowing for consistent reimbursement rates and comparisons between hospitals. Each DRG has a specific payment weight associated with it, determining the reimbursement for the entire hospital stay, regardless of the actual costs incurred.
Use of DRG Codes
DRG codes play a pivotal role in the hospital reimbursement process, as they determine the payment for inpatient services rendered. Insurance companies, including Medicare and Medicaid, utilize DRG codes to calculate reimbursement rates based on the patient’s diagnosis, procedures performed, age, and other factors. Additionally, DRG codes facilitate benchmarking and outcome analysis, enabling hospitals to evaluate their performance and make data-driven improvements.
Examples of DRG Codes
DRG codes cover a broad range of medical conditions and procedures. Here are a few examples of DRG codes:
DRG 247 – Percutaneous cardiovascular procedures with drug-eluting stent with medically managed acute myocardial infarction
DRG 392 – Esophagitis, gastroent, misc digest disorders with major gastrointestinal procedure with CC
DRG 456 – Spinal fusions except cervical with spinal curvature or malignancy or infection or extensive fusion of the spine
DRG 637 – Diabetes with complication, age > 35 with complications with major CC
DRG 811 – Red blood cell disorders with MCC
Modifiers
Importance of Modifiers in Medical Coding
Modifiers are essential components of the medical coding system as they provide additional information to clarify the nature and extent of a medical service or procedure. These two-digit codes are added to the main procedure or service code to indicate specific circumstances, such as multiple procedures, altered anatomical sites, or distinct levels of service. Modifiers play a critical role in ensuring accurate billing, communication between healthcare providers, and appropriate reimbursement determination.
Common Modifiers
Modifiers are categorized into various groups and subsets, each serving a specific purpose. Some commonly utilized modifiers include:
-25: Significant, separately identifiable evaluation and management service by the same physician on the same day of a procedure or other service.
-59: Distinct procedural service, indicating that a procedure or service is independent of another service performed on the same day.
-TC: Technical component, indicating that only the technical aspect of a service or procedure was performed.
-RT/-LT: Right side/left side, indicating that a procedure or service was performed on a specific side of the body.
Examples of Modifier Usage
Here are a few examples to illustrate the usage of modifiers in medical coding:
99213-25 – Office visit – established patient, significant, separately identifiable evaluation and management service on the same day as a procedure
29881-59 – Arthroscopy, knee, surgical; with meniscectomy, medial and lateral, including any meniscal shaving
93880-TC – Duplex scan of extracranial arteries; complete bilateral study
27829-RT – Open treatment of patellar fracture, with internal fixation, right patella
Definition of Evaluation and Management (E&M) Coding
Evaluation and Management (E&M) coding refers to the process of assigning codes to patient encounters or visits that involve the evaluation, examination, and management of a patient’s medical condition. E&M codes reflect the level of complexity, medical decision-making, and documentation required for the encounter. These codes are vital for billing purposes, determining reimbursement, and communicating the severity of the patient’s condition to other healthcare professionals.
Components of E&M Coding
E&M codes consider various components to determine the appropriate level of service. The key components include:
History: Assessing the patient’s symptoms, medical background, and pertinent details related to the current visit.
Examination: Performing a relevant physical examination to assess the patient’s condition systematically.
Medical Decision-Making: Evaluating the complexity of the patient’s condition, considering factors such as diagnosis, treatment options, risk, and follow-up requirements.
Time: Considering the total time spent on the encounter, including face-to-face time with the patient and any additional work performed outside the encounter.
Examples of E&M Codes
Here are examples of E&M codes that represent different levels of service:
99202 – Office visit – new patient, low complexity, with a detailed history, expanded problem-focused examination, straightforward medical decision-making
99213 – Office visit – established patient, moderate complexity, with an expanded problem-focused history, expanded problem-focused examination, straightforward medical decision-making
99285 – Emergency department visit – moderate to high complexity, with a comprehensive history, comprehensive examination, medical decision-making of moderate complexity
99245 – Office consultation – new or established patient, comprehensive history, comprehensive examination, high complexity medical decision-making, face-to-face time over 60 minutes
Anesthesia Codes
Overview of Anesthesia Coding
Anesthesia coding involves assigning codes to the administration of anesthesia during surgical or medical procedures. Anesthesia services are essential to ensure patient comfort and safety during invasive or painful interventions. Proper coding of anesthesia services allows for accurate billing, appropriate reimbursement, and documentation of the specific anesthesia techniques employed.
Types of Anesthesia Codes
Anesthesia codes can be divided into three main categories based on the type of anesthesia provided:
General Anesthesia: Codes for general anesthesia indicate a state of drug-induced unconsciousness, pain control, and muscle relaxation throughout the entire procedure.
Regional Anesthesia: These codes represent the injection or infusion of anesthetic agents to block specific nerve impulses, rendering a specific area of the body temporarily numb.
Monitored Anesthesia Care: Codes for monitored anesthesia care signify anesthesia services provided for procedures that do not require general or regional anesthesia. These services involve the administration of sedation or analgesia, with continuous patient monitoring.
Examples of Anesthesia Codes
Here are examples of anesthesia codes representing various types:
00300 – Anesthesia for procedures on integumentary system of one extremity, not otherwise specified
01991 – Monitored anesthesia care for patient of extreme age, younger than 1 year and older than 70 years, first 30 minutes
00532 – Anesthesia for open or surgical arthroscopic procedures on knee joint; with gastrocnemius recession
01967 – Neuraxial labor analgesia/anesthesia for planned vaginal delivery, including any associated induction or augmentation
01404 – Anesthesia for pharyngeal surgery
Radiology Codes
Introduction to Radiology Coding
Radiology coding involves classifying and assigning codes to medical imaging procedures, such as X-rays, CT scans, MRIs, and ultrasounds. These procedures are vital for diagnosing and monitoring various medical conditions. Accurate and detailed coding of radiology services ensures proper billing, facilitates reimbursement, and supports effective communication among healthcare professionals.
Types of Radiology Codes
Radiology codes cover a wide range of imaging procedures across different modalities. Some common types of radiology codes include:
Radiologic Supervision and Interpretation (RS&I): Codes for RS&I encompass the professional interpretation of radiologic images and supervision of the technical aspects of the radiology procedure.
Diagnostic Radiology: These codes represent the technical component of the radiology procedure, including the use of specific equipment and techniques for image acquisition.
Interventional Radiology: Codes for interventional radiology cover procedures that involve the use of radiological guidance to perform minimally invasive therapeutic or diagnostic interventions.
Examples of Radiology Codes
Here are examples of radiology codes across different modalities and procedures:
70553 – MRI brain, without contrast, followed by contrast
74183 – CT abdomen and pelvis; without contrast material and without contrast material in certain specified clinical scenarios
76805 – Ultrasound, pregnant uterus, real-time with image documentation, fetal and maternal evaluation, second and third trimesters
76000 – Fluoroscopy, physician time more than one hour, assisting a non-radiologic physician
Pathology and Laboratory Codes
Understanding Pathology and Laboratory Coding
Pathology and Laboratory coding involves assigning codes to various laboratory tests, procedures, and services performed on patient specimens. These codes capture essential diagnostic, therapeutic, and monitoring elements required for providing comprehensive healthcare. Accurate coding of pathology and laboratory services enables effective communication, billing, and reimbursement for the diagnostic and analytical services provided.
Types of Pathology and Laboratory Codes
pathology and laboratory codes cover a broad spectrum of tests and services offered in the clinical laboratory setting. Some common categories of Pathology and Laboratory codes include:
Laboratory Panels: Codes representing a comprehensive group of laboratory tests commonly performed together to screen for specific diseases or conditions.
Molecular Pathology: These codes cover molecular diagnostic testing, including DNA/RNA analysis, genetic testing, and other molecular profiling techniques.
Special Stain and IHC: Codes for special stains and immunohistochemistry (IHC) allow for the identification and characterization of specific cellular components and molecular markers.
Microbiology: Microbiology codes include tests and services related to the detection, identification, and susceptibility testing of microorganisms, such as bacteria, viruses, and fungi.
Examples of Pathology and Laboratory Codes
Here are examples of pathology and laboratory codes across different categories:
80050 – General health panel – comprehensive metabolic panel (CMP) and complete blood count (CBC)
88305 – Surgical pathology, gross and microscopic examination, for each tissue or organ biopsy; with routine H&E stain(s)
81479 – Unlisted molecular pathology procedure, not otherwise specified
87081 – Bacterial culture, aerobic, with isolation and presumptive identification of isolates
88342 – Immunohistochemistry or immunocytochemistry, per specimen; each antibody separately identified
In conclusion, medical coding is a critical process in healthcare, ensuring standardized documentation, accurate billing, and effective communication. Understanding the basics of coding systems, such as ICD-10-CM, CPT codes, HCPCS codes, DRG codes, modifiers, E&M coding, anesthesia codes, radiology codes, and pathology and laboratory codes, is essential for healthcare professionals involved in coding and billing procedures. accurate and comprehensive coding helps streamline healthcare operations, supports reimbursement, improves patient care, and facilitates data analysis for research and quality improvement initiatives.